All-Inclusive Guide to Autohemotherapy: Essential Information
People are constantly searching for alternative therapies that support the body's inherent healing capacity in their pursuit of well-being. The intriguing and becoming more well-liked therapy known as autohemotherapy is drawing interest due to its ability to improve vitality and health. We'll go into the specifics of autohemotherapy in this extensive guide, answering any questions you may have about this fascinating healing modality.
Knowing About Autohemotherapy:
**1. Foundations:**
Reinfusion of a patient's own blood—which has undergone some sort of modification or treatment—into the body is known as autohemotherapy. Numerous physiological reactions are triggered by this process, which might have a favorable effect on one's general health and well-being.
**2. Distinct Methods:**
There are several variations of autohemotherapy, and each has special advantages. People can select a technique that suits their interests and health goals from a variety of possibilities, such as major autohemotherapy, UV light therapy, and Ozone Autohemotherapy, which involves treating blood with medical-grade ozone.
**3. Increased Oxygenation:**
The rise in blood oxygen levels is one of the main advantages of autohemotherapy. This therapy enhances cellular activity and helps the body function at its peak by enhancing oxygenation.
**4. Modulation of the Immune System:**
Immune system modulation has been associated with autohemotherapy, which strengthens the body's defense mechanisms. Because of this, it's a very appealing choice for people who want to boost their immunity against diseases and infections.
What to anticipate:
**1. Professional Consultation:**
It's important to speak with a healthcare provider before beginning autohemotherapy. They will review your goals, evaluate your medical history, and choose the best course of action based on your particular requirements.
**2. Therapy Meetings:**
The chosen method and the specific health conditions of each patient may influence the frequency and length of Autohemotherapy sessions. Most people indicate that their sessions are generally well-tolerated, with only minor discomfort.
**3. Possible Advantages:**
Enthusiasts of autohemotherapy have documented a number of advantages, such as heightened vitality, enhanced immunity, and overall wellbeing. But it's important to remember that every person will react differently.
### Safety Points to Remember:
Professional Oversight: **1.
Only qualified medical personnel should oversee the administration of autohemotherapy. Unsupervised therapies or do-it-yourself methods carry potential dangers and should be avoided.
**2. Personalized Approach:** Reactions to autohemotherapy can differ between individuals and health situations. Working with medical experts who can customize the treatment plan to meet your unique needs is therefore essential.
For those looking for a natural and comprehensive approach to wellbeing, autohemotherapy appears to be a viable option. Through comprehension of the fundamentals, investigation of various methods, and assessment of safety issues, people can make knowledgeable choices on the incorporation of Autohemotherapy into their health journey. To ensure a safe and successful experience, like with any health-related decision, consulting with healthcare specialists is essential. Take advantage of autohemotherapy's potential advantages and set out on a journey to improved health and vigor!
Accepting Well-Being: Exposing the Advantages of Ozone Autohemotherapy
People are always looking into cutting-edge therapies that use the power of nature in their quest for holistic health and wellness. Ozone Autohemotherapy is one such therapy that is gaining popularity. It is a method that involves injecting ozone into one's own blood for a host of health advantages. We'll explore the intriguing field of ozone autohemotherapy in this blog and see how it may be able to open the door to a happier, healthier existence.
Recognizing Ozone for Autohemotherapy: A little portion of a patient's blood is removed during autohemotherapy, which is a minimally invasive technique. The blood is then treated with medical-grade ozone and reintroduced into the body. This process promotes general well-being by inducing a variety of physiologic reactions.
Enhanced Oxygenation: The molecule ozone, which is made up of three oxygen atoms, has the amazing capacity to raise the body's oxygen content. Ozonated blood supports cellular function and vitality by delivering increased concentrations of oxygen to tissues and organs when it enters the bloodstream.
Ozone: Enhanced Immune System It is well known that autohemotherapy modulates the immune system, increasing its effectiveness in fending against infections and illnesses. Ozone helps the body create a stronger barrier against infections by stimulating immune cells, which in turn strengthens the body's inherent healing capacity.
Detoxification: The body may eliminate toxins and metabolic waste products with the help of ozone's potent detoxifying qualities. The liver and kidneys are supported during this detoxification process, which also fosters a healthier, more hygienic internal environment.
Anti-Inflammatory Effects: A number of health problems are preceded by chronic inflammation. Ozone contributes to a more balanced and harmonious body state by having anti-inflammatory qualities that can help reduce inflammation and lower the risk of inflammatory-related illnesses.
Ozone Promotes Better Circulation There is evidence that autohemotherapy promotes better blood circulation. This treatment may improve the transport of nutrients and oxygen to cells, facilitating tissue regeneration and repair, by increasing blood flow.
Pain management: Ozone autohemotherapy may be able to provide relief for people with long-term pain issues. The analgesic and anti-inflammatory properties of the therapy can help control pain and enhance quality of life in general.
The use of ozone (O3) gas as a therapy in alternative medicine has attracted skepticism due to its unstable molecular structure. However, copious volumes of research have provided evidence that O3's dynamic resonance structures facilitate physiological interactions useful in treating a myriad of pathologies. Specifically, O3 therapy induces moderate oxidative stress when interacting with lipids. This interaction increases endogenous production of antioxidants, local perfusion, and oxygen delivery, as well as enhances immune responses. We have conducted a comprehensive review of O3 therapy, investigating its contraindications, routes and concentrations of administration, mechanisms of action, disinfectant properties in various microorganisms, and its medicinal use in different pathologies. We explore the therapeutic value of O3 in pathologies of the cardiovascular system, gastrointestinal tract, genitourinary system, central nervous system, head and neck, musculoskeletal, subcutaneous tissue, and peripheral vascular disease. Despite compelling evidence, further studies are essential to mark it as a viable and quintessential treatment option in medicine.
Ozone (O3) gas was discovered in the 1840s, and soon after that, the scientific community began to expand past the notion that it was just another gas of the Earth's atmosphere. Though the migration of O3 into the medical field has taken a circuitous road since the 19th century, its medicinal value is currently controversial despite compelling research.1 O3 is highly water-soluble inorganic molecule composed of three oxygen molecules. O3's inherently unstable molecular structure, due to the nature of its mesomeric states, tends to make it difficult to obtain high concentrations. O3 will often experience transient reactions with itself or water. Thus, it was initially problematic to achieve desired levels and even more difficult is to assess the therapeutic effects of such a transient state.1,2 These mesomeric states create a conundrum within the scientific community. A divide has formed between those who believe the volatile nature of these mesomeric states can foster positive responses and those who are wary of its seemingly dangerous effects.
Despite suspicions, a multitude of O3 therapies have shown substantial benefits that span a large variety of acute and chronic ailments. O3 is currently prevalent in dentistry to treat diseases of the jaw.1 O3 has also proven itself beneficial as a disinfectant for drinking water and sterilization of medical instruments.1,3 The function of O3 shares similarities to that of a prodrug, as it is modified upon reacting with molecules to create more active substrates, thus stimulating an endogenous cascade of responses. On the other hand, it is hard to classify O3 as simply a prodrug, due to its capability to directly interact with phospholipids, lipoproteins, cell envelopes of bacteria, and viral capsids. The physiology of these biological responses is herein discussed.
Despite the various benefits, O3 toxicity and clinical utility depends on the concentration and administration to the appropriate site.1,2,4,5 One of the major contraindications of O3 therapy is lung inhalation. O3 therapy significantly increases airway resistance without changing the compliance or elastic characteristics of the lung.1 Additionally, direct contact of O3 with the eyes and lungs is contraindicated because of the low antioxidant capabilities in these specific locations.6
A MEDLINE® database search of literature extended from 1980 to 2017 to obtain current information regarding O3 therapy, its routes of administration, and mechanism of action. Subsequently, trials pertaining to the clinical implications of O3 therapy were paired by pathology and anatomical system. The most important points refer to the type of pathology, route of O3 administration, type of research trial, result(s) of the trial, side effect(s), and proposed physiological mechanism(s). Literature retrieval was performed in July 2017 and included the term “ozone therapy” combined with the following search criteria: “routes of administration”, “mechanism of action”, “cardiovascular”, “subcutaneous tissue”, “peripheral vascular disease”, “neurological”, “head and neck”, “orthopedic”, “musculoskeletal”, “gastrointestinal”, and “genitourinary”. We did not formulate any exclusion criteria.
O3 therapy combines a mixture of oxygen (O2)-O3, with a diverse therapeutic range (10–80 μg/ml of gas per ml of blood).5,6,7 O3 therapy administration is variable based on treatment goals and location of therapy. The first and most popular is O3 autohemotransfusion (O3-Aht). O3-Aht has grown in popularity because it allows for a predetermined amount of blood to be taken and thus, using stoichiometric calculations, a precise concertation of O2-O3 can be infused. This small amount of blood is subjected to O2-O3ex vivo is then administered to the patient.5,6 Extracorporeal blood oxygenation and ozonation are very similar techniques. However, its goal is to obtain higher blood volume than the 200–300 mL seen in O3-Aht.5
Other modalities of therapies include direct injection via the intramuscular, intradiscal, and paravertebral site of administration. Rectal insufflation of O3-O3 is another common site of administration. However, insufflation of the nasal, tubal, oral, vaginal, vesical, pleural, and peritoneal cavities have proven to be prudent routes of administration. Cutaneous exposure has also had likely outcomes and can be achieved by sealing the portion of the body in a chamber or bag and insufflating with O3-O3 mixture. Saline with O3-O3 dissolved is used to avoid the risk of embolism when administered intravenously.5
Upon beginning O3 therapy, a multifaceted endogenous cascade is initiated and releases biologically active substrates in response to the transient, and moderate, oxidative stress that O3 induces. O3 can cause this mild oxidative stress because of its ability to dissolve in the aqueous component of plasma.8 By reacting with polyunsaturated fatty acids (PUFA) and water, O3 creates hydrogen peroxide (H2O2), a reactive oxygen species (ROS). Simultaneously, O3 forms a mixture of lipid ozonation products (LOP).9 The LOPs created after O3 exposure include lipoperoxyl radicals, hydroperoxides, malonyldialdeyde, isoprostanes, the ozonide and alkenals, and 4-hydroxynonenal (4-HNE). Moderate oxidative stress caused by O3 increases activation of the transcriptional factor mediating nuclear factor-erythroid 2-related factor 2 (Nrf2). Nrf2's domain is responsible for activating the transcription of antioxidant response elements (ARE). Upon induction of ARE transcription, an assortment of antioxidant enzymes gains increased concentration levels in response to the transient oxidative stress of O3. The antioxidants created include, but are not limited to, superoxide dismutase (SOD), glutathione peroxidase (GPx), glutathione S-transferase (GST), catalase (CAT), heme oxygenase-1 (HO-1), NADPH-quinone-oxidoreductase (NQO-1), heat shock proteins (HSP), and phase II enzymes of drug metabolism. Many of these enzymes act as free radical scavengers clinically relevant to a wide variety of diseases.9
O3, as well as other medical gases, e.g., carbon monoxide (CO) and nitric oxide (NO), has twofold effects depending on the amount given and the cell's redox status. There is a complex relationship between these three medical gases as O3 overexpresses HO-1, also referred to as HSPs of 32 kPa (Hsp32),10 the enzyme responsible for CO formation, and downregulates NO synthase, which generates NO. Furthermore, O3 upregulates the expression levels of Hsp70 which, in turn, is strictly related to HO-1. O3 may have a developing role in Hsp-based diagnosis and therapy of free radical-based diseases. HO-1 degrades heme, which can be toxic depending on the amount produced, into free iron, CO, and biliverdin (i.e., precursor of bilirubin), a neutralizer of oxidative and nitrosative stress due to its ability to interact with NO and reactive nitrogen species.11,12 Recently, it is becoming clear the heat shock response (HSR) provides a cytoprotective state during inflammation, cancer, aging, and neurodegenerative disorders.13 Given its extensive cytoprotective properties, the HSR is now a target for induction via pharmacological agents.1 Hsp70 is involved in co- and post-translational folding, the quality control of misfolded proteins,14 folding and assembly of de novo proteins into macromolecular complexes, as well as anti-aggregation, protein refolding, and degradation.15 HO isoforms are acknowledged as dynamic sensors of cellular oxidative stress and regulators of redox homeostasis throughout the phylogenetic spectrum. The effect of O3 on these cell activities remains to be evaluated. Hormesis is a potent, endogenous defense mechanism for lethal ischemic and oxidative insults to multiple organ systems.13 O3 may have a hormetic role in regulating the anti-inflammatory and proinflammatory effects of CO, including prostaglandin formation akin to NO, which has been shown to exert some of its biological actions through the modulation of prostaglandin endoperoxide synthase activity.16 Inhibiting HO activity prevents CO biosynthesis and its downstream effects17; the effect of O3 on this cascade is yet to be determined.
Animal models have postulated the beneficial effects of prophylactic O3 therapy in controlling the age-related effects of oxidative stress.18,19 Evidence was provided to show that low O3 dose administration provided beneficial effects on age-related alterations in the heart and hippocampus of rats. Additional research has been performed and provided room for speculation that O3 therapy may provide the mediation of a mechanism involved in rebalancing the dysregulated redox state that accumulates as individuals age.20 There was an apparent reduction of lipid and protein oxidation markers, lessening of lipofuscin deposition, restoration of glutathione (GSH) levels, and normalization of GPx activity in aged heart tissue. O3 was demonstrated to decrease age-associated energy failure in the heart and hippocampus of rats. Researchers suspect that the improved cardiac cytosolic calcium and restoration of weakened Na+-K+ ATPase activity in the heart and hippocampus, respectively, were associated with the improvements seen.20
In hopes of attaining a sense of the possible toxic components of O3 therapy, a study was done to assess the extent of lesions on human hematic mononucleated cells (HHMC), human thymic epithelium, murine macrophages, mouse splenocytes, and B16 melanoma murine cells. A significant finding of the study was that Hsp70 exhibited an O3-induced increase in biosynthesis in HHMC. Hsp70s are synthesized in response to thermal shock and other stressing agents to cope with the damage that stimulates their biosynthesis.21 Additionally, they stimulate several immune system responses in lymphocytes and macrophages. The study provided evidence that O3 is a stressing agent capable of upregulating the biosynthesis of Hsp70, without toxicity to membranes. However, the membranes of macrophages are highly resistant to the possible toxicity of O3 at high concentrations; HHMC is less resistant at the high end of the spectrum. The statement above should not discount the effectiveness of O3 as a therapy because Hsp70s are induced in HHMCs without lesions up to 20 μg/mL— a typical dose given in O3-AHT.21
Cisplatin (CDDP), a treatment used in a variety of cancers has been observed to have nephrotoxicity in 25% of the patients as a side effect. The occurrence of this nephrotoxicity is thought to be secondary to the free radical generation and the inability of ROS scavengers to ameliorate these molecules, leading to acute renal failure. O2-O3 therapy was used to increase the antioxidant capacity of rats exposed to CDDP and compared to control groups. Serum creatine levels were significantly reduced compared to control groups, illustrating the decreased nephrotoxicity indirectly in the rats with CDDP and O2-O3 therapy. In addition to attenuating the nephrotoxicity, O2-O3 therapy also restores the levels of antioxidant defense constituents (GSH, SOD, CAT, and GSH-Px), which are usually decreased by CDDP. Also, thiobarbituric acid reactive substances (TBARS) were reduced, which is a marker of lipid peroxidation in the kidney.22,23
Additional human studies examined the beneficial effects of O3 therapy employed via O3-AHT, in conjunction with coenzyme Q10, administered orally. The study evaluated SOD levels, a powerful antioxidant and catalase enzyme, an additional antioxidant enzyme in a control group, a group of O3 therapy by itself, and O3 therapy combined with Q10. Evidence has implied that SOD was significantly increased and catalase enzyme insignificantly increased in the O3 + Q10 group when compared to the control group. Malondialdehyde, a product of lipid peroxidation, is an indicator of oxidative membrane damage. Malondialdehyde levels were significantly decreased concentrations in the O3 + Q10 group when compared to the control group. Taken together, this study provides evidence of the beneficial effects of O3 therapy in combination with Q10 in combatting and the prevention of damage elicited by oxidation.9
Multiple studies have provided evidence that O3 therapy increased activation of the Nrf2 pathway via the induction of moderate oxidative stress.15,24 By doing so, a transient increase in H2O2 and LOPs enhances the number of antioxidants and therefore can be used for a longer time frame to re-establish the balance of the redox system. Additionally, the creation of these antioxidant enzymes has effects, not only at the level of O3 radical metabolism, but on the whole body.22,23
Researchers have argued that knowing the total antioxidant status and plasma protein thiol group levels of a blood sample are indicators of the precise amount of O3 required to optimize treatments. By developing more accurate antioxidant status indicators, an individual treatment would achieve the correct dosage on a day and case basis.7,23,25 Systems have been proposed to have a more precise measurement of the redox state of a patient to achieve this goal. One system proposes simultaneously measuring different biological markers in the blood such as GSH, GPx, GST, SOD, CAT, conjugated dienes, total hydroperoxides, and TBARS. Using an algorithm, information can be gathered about the total antioxidant activity, total pro-oxidant activity, redox index, and grade of oxidative stress. Systems like this can provide insights to the correct dosage and response to O3 therapy based on oxidative stress levels seen in the patient.7,23,25
Vascular and hematological modulation
O3 is a stimulator of the transmembrane flow of O2. The increase in O2 levels inside the cell secondary to O3 therapy makes the mitochondrial respiratory chain more efficient.26 In red blood cells, O3-AHT may increase the activity of phosphofructokinase, increasing the rate of glycolysis. By enhancing the glycolytic rate, there is an increase in ATP and 2,3-diphosphoglycerate (2,3-DPG) in the cell. Subsequently, due to the Bohr effect, there is a rightward shift in the oxyhemoglobin dissociation curve allowing for the oxygen bound hemoglobin to be unloaded more readily to ischemic tissues. Combined with the increase in NO synthase activity, there is a marked increase in perfusion to the area under stimulation by O3-AHT.27 With repeated treatment, sufficient enough LOP may be generated to reach the bone marrow acting as repeated stressors to simulate erythrogenesis and the upregulation of antioxidant enzyme upregulation. O3 also causes a reduction in nicotinamide adenine dinucleotide (NADH) and assists in the oxidation of cytochrome c.1,28
O3 has also been shown to improve blood circulation and oxygen delivery to ischemic tissues.29 Multiple studies have provided evidence that the correction of chronic oxidative stress via the increase of antioxidant enzymes in O3 can increase erythroblast differentiation. This leads to a progressive increase in erythrocytes and preconditions them to having resilience towards oxidative stress. This is known as “oxidative preconditioning”.1,30 Also, O3 increases levels of prostacyclin, a known vasodilator.1
Additionally, it was speculated that O3's oxidative capabilities would interfere with the endothelial production of NO and thus hinder vasodilation. However, studies have provided evidence that because NO is not substantially transported in the vasculature of the blood, a deleterious interaction is unlikely.29 Since HO-derived bilirubin31 has been demonstrated to interact with NO,11,12 O3-induced HO upregulation could modify NO production and alter vasodilation.
Unpredictably, studies have shown an increase of NO, which led to speculation of O3's ability to activate genes associated with NO synthase expression to further promote higher levels of NO formation. Moreover, O3's stimulation of antioxidant enzymes are also speculated to increase NO levels. While endothelial generation of superoxide disrupts the activity of NO, O3 upregulates the enzymes to ameliorate the downstream effects of ROS responsible for deleterious vasoconstriction.29,32
The prophylactic role of O3 has been explored with hepatic ischemia/reperfusion (I/R) injury, a phenomenon associated with liver transplantation. Hepatic I/R is a clinically unsolved problem mainly due to the unknown mechanisms that are the foundations of this ailment. In summary, O3 oxidative preconditionings (ozoneOPs) were found to protect against liver I/R injury through mechanisms that promote a regulation of endogenous NO concentrations and the maintenance of an adequate cellular redox balance. OzoneOPs are postulated to upregulate endogenous antioxidant systems and generate an increase in NO molecule generation, both of which are protective orders against liver and pancreas damage. The results in this animal model provided evidence that ozoneOPs protected against liver I/R via an increase in concentrations of endogenous NO and prime cells to have a more balanced redox system.32 Additionally, enhanced activation of adenosine A1 receptors in rat models have been observed with ozoneOPs in liver I/R.33
Further studies have expanded upon this postulation by applying O3 therapy to renal I/R in rats. Renal I/R is a primary cause of acute renal failure after transplantation surgery. The findings of a study by Orakdogen et al.34 indicated that the ozoneOPs allowed for a protective element when facing I/R. Following an increase in endothelial NO synthase and inducible NO synthase expression, it was concluded that ozoneOPs were intimately related to the increasing NO production as well as reducing renal damage by suppressing endothelin 1.34
Cerebral vasospasm after subarachnoid hemorrhage is a significant detriment to the recovery of patients. An animal model examined the effects intravenous O3 therapy on vasospasms in the rat femoral artery. Histopathological and morphometric measurements provided evidence that O3 therapy decreased morphometric changes, disruption of endothelial cells, and hemorrhages that are a result of vasospasm. The study speculated the anti-oxidative and anti-inflammatory effects of O3 might be a prudent treatment for posthemorrhagic vasospasm.35
Pathogen inactivation
When bacteria are exposed to O3in vitro, the phospholipids, and lipoproteins that are within the bacterial cell envelope are oxidized. As this occurs, the stability of the bacterial cell envelope is attenuated. Moreover, evidence has demonstrated O3 to interact with fungal cell walls like bacteria. This disrupts the integrity of the cytosolic membrane and infiltrates the microorganisms to oxidize glycoproteins, glycolipids, and block enzymatic function. The combination of these reactions causes inhibition of fungi growth and mortality of bacteria and fungi.1,3,5In vitro, O3 has been shown to interfere with virus-to-cell contact in lipid-enveloped viruses via oxidation of lipoproteins, proteins, and glycoproteins, thus interfering with the viral reproductive cycles.1,3,36
Specifically, animal models have shown that O3 therapy as an adjunct to vancomycin enhances the animal's capability to eliminate methicillin-resistant Staphylococcus aureus mediastinitis.37
Immune system activation
In vivo, O3 therapy has been shown to have multifaceted effects when interacting with PUFA. As stated previously, O3 reacts with PUFA and other antioxidants, H2O2 and varies peroxidation compounds are formed. H2O2 readily diffuses into immune cells has been shown to act as a regulatory step in signal transduction and facilitating a myriad of immune responses.36,38 Specifically, increases in interferon, tumor necrosis factor, and interleukin (IL)-2 are seen. The increases with IL-2 are known to initiate immune response mechanisms.1 Additionally, H2O2 activates nuclear factor-kappa B (NF-κB) and transforming growth factor beta (TGF-β), which increase immunoactive cytokine release and upregulate tissue remodeling. H2O2 mediates the action of NF-κB by enhancing the activity of tyrosine kinases that will phosphorylate IκB, a subunit of the transcription factor NF-κB.34,37 Low doses of O3 have been shown to inhibit prostaglandin synthesis, release bradykinin, and increase secretions of macrophages and leukocytes.34 Having the correct amount of either of these oxidative markers can be used to create a sufficient rise in H2O2 and NO levels to stimulate the most notable increase in IL-8. IL-8 also activates NF-κB, allowing production of ROS scavengers.7
Animal models using O3 have shown to reduce and prevent inflammatory responses steming from the presence of E. coli in the renal system.26,38 Additional studies have provided evidence of the anti-inflammatory effects of O3. A study by Chang et al.25 purified rheumatoid arthritis synovial fibroblast cells from human patients and injected them into immunocompromised mouse joints. Using an Ozonsan-α generator to deliver precise gas flows to vessels in the localized area, the authors discovered that 3% and 5% O3 application significantly decreased the proinflammatory cytokines IL-1β, IL-6, and TNF-α without any toxicity or severe side effects.25
Studies have shown that human cancer cells from lung, breast, and uterine tumors are inhibited in a dose-dependent manner by O3 therapy in vitro. O3 concentrations of 0.3 and 0.5 ppm inhibited cancer cell growth by 40% and 60%, respectively. Furthermore, the noncancerous cell controls were not affected by these levels of O3. At 0.8 ppm, cancer cell growth was inhibited by more than 90%. However, the control cell growth was less than 50%. Additionally, as control cells aged, they exhibited further growth inhibition and morphological changes. The study speculated that as the healthy cells matured, there was a decrease in growth due to the increased cellular damage incurred by each division.39
With its ever-growing ubiquity, O3 therapy is finding a place in many branches of medicine and medical specialties. In fact, its clinical use can be arranged systematically into cardiovascular (Additional Table 1), subcutaneous tissue (Additional Table 2), peripheral vascular disease (Additional Table 3), neurological (Additional Table 4), head and neck (Additional Table 5), orthopedic (Additional Table 6), gastrointestinal (Additional Table 7), and genitourinary (Additional Table 8). These indications are a product of human clinical trials conducted for specific pathologies related to the aforementioned systems. Despite a lack of direct support of O3 therapy, the current Food and Drug Administration regulations do not restrict the use of it in situations where it has proven its safety and effectiveness. Nonetheless, there has been support for its safety and effectiveness in multi-international studies.
O3 therapy can alter the natural history of several disease and disorders, with potentially many more yet untested. A plethora of laboratory studies have provided evidence of O3's antioxidant capabilities, as well as vascular, hematological, and immune system modulations. This evidence has been further substantiated in clinical trials with O3 therapy being useful in the cardiovascular, subcutaneous tissue, peripheral vascular disease, neurological, head and neck, orthopedic, gastrointestinal, and genitourinary pathologies. O3 therapy has proven especially beneficial in the diabetic foot, ischemic wounds, and peripheral vascular disease, areas in which O3 use is most prevalent. Upcoming laboratory and translational research should begin to develop protocols for O3-AHT in attempts to establish a dose-response relationship as it has demonstrated high utility in a myriad of pathologies at varying concentrations. Despite the presently compelling evidence, future studies should include more double-blind, randomized clinical trials with greater sample sizes, determination of longevity in benefits produced, as well as methods of measurements and analysis.
The authors are thankful to Drs. Kelly Warren, Inefta Reid, Todd Miller, and Peter Brink (Department of Physiology and Biophysics, Stony Brook University School of Medicine, Stony Brook, NY, USA) for departmental support, as well as Mrs. Wendy Isser and Ms. Grace Garey (Northport VA Medical Center Library, Northport, NY, USA) for literature retrieval.
The authors have no conflicts of interest to declare.
Plagiarism check
Checked twice by iThenticate.
Peer review
Externally peer reviewed.
Open peer reviewers
Ozan Akca, University of Louisville, USA; Nemoto Edwin, University of New Mexico Health Sciences Center, USA; Mancuso Cesare, Università Cattolica del Sacro Cuore, Italy.
2. Zanardi I, Borrelli E, Valacchi G, Travagli V, Bocci V. Ozone: a multifaceted molecule with unexpected therapeutic activity. Curr Med Chem. 2016;23:304–314. [PubMed] [Google Scholar]
3. Azarpazhooh A, Limeback H. The application of ozone in dentistry: a systematic review of literature. J Dent. 2008;36:104–116. [PubMed] [Google Scholar]
4. Bocci VA. Tropospheric ozone toxicity vs. usefulness of ozone therapy. Arch Med Res. 2007;38:265–267. [PubMed] [Google Scholar]
5. Bocci VA. Scientific and medical aspects of ozone therapy. State of the art. Arch Med Res. 2006;37:425–435. [PubMed] [Google Scholar]
6. Bocci V. Autohaemotherapy after treatment of blood with ozone. A reappraisal. J Int Med Res. 1994;22:131–144. [PubMed] [Google Scholar]
7. Bocci V, Valacchi G, Corradeschi F, Fanetti G. Studies on the biological effects of ozone: 8. Effects on the total antioxidant status and on interleukin-8 production. Mediators Inflamm. 1998;7:313–317. [PMC free article] [PubMed] [Google Scholar]
8. Bocci V, Larini A, Micheli V. Restoration of normoxia by ozone therapy may control neoplastic growth: a review and a working hypothesis. J Altern Complement Med. 2005;11:257–265. [PubMed] [Google Scholar]
9. Inal M, Dokumacioglu A, Ozcelik E, Ucar O. The effects of ozone therapy and coenzyme Q(1)(0) combination on oxidative stress markers in healthy subjects. Ir J Med Sci. 2011;180:703–707. [PubMed] [Google Scholar]
10. Bocci V, Aldinucci C, Mosci F, Carraro F, Valacchi G. Ozonation of human blood induces a remarkable upregulation of heme oxygenase-1 and heat stress protein-70. Mediators Inflamm. 2007;2007:26785. [PMC free article] [PubMed] [Google Scholar]
11. Mancuso C, Capone C, Ranieri SC, et al. Bilirubin as an endogenous modulator of neurotrophin redox signaling. J Neurosci Res. 2008;86:2235–2249. [PubMed] [Google Scholar]
12. Barone E, Trombino S, Cassano R, et al. Characterization of the S-denitrosylating activity of bilirubin. J Cell Mol Med. 2009;13:2365–2375. [PMC free article] [PubMed] [Google Scholar]
13. Dattilo S, Mancuso C, Koverech G, et al. Heat shock proteins and hormesis in the diagnosis and treatment of neurodegenerative diseases. Immun Ageing. 2015;12:20. [PMC free article] [PubMed] [Google Scholar]
14. Martínez-Sánchez G, Delgado-Roche L, Díaz-Batista A, Pérez-Davison G, Re L. Effects of ozone therapy on haemostatic and oxidative stress index in coronary artery disease. Eur J Pharmacol. 2012;691:156–162. [PubMed] [Google Scholar]
15. Bocci V, Valacchi G. Nrf2 activation as target to implement therapeutic treatments. Front Chem. 2015;3:4. [PMC free article] [PubMed] [Google Scholar]
16. Mancuso C, Pistritto G, Tringali G, Grossman AB, Preziosi P, Navarra P. Evidence that carbon monoxide stimulates prostaglandin endoperoxide synthase activity in rat hypothalamic explants and in primary cultures of rat hypothalamic astrocytes. Brain Res Mol Brain Res. 1997;45:294–300. [PubMed] [Google Scholar]
17. Navarra P, Dello Russo C, Mancuso C, Preziosi P, Grossman A. Gaseous neuromodulators in the control of neuroendocrine stress axis. Ann N Y Acad Sci. 2000;917:638–646. [PubMed] [Google Scholar]
18. Onal O, Yetisir F, Sarer AE, et al. Prophylactic ozone administration reduces intestinal mucosa injury induced by intestinal ischemia-reperfusion in the rat. Mediators Inflamm. 2015;2015:792016. [PMC free article] [PubMed] [Google Scholar]
19. Kal A, Kal O, Akillioglu I, et al. The protective effect of prophylactic ozone administration against retinal ischemia-reperfusion injury. Cutan Ocul Toxicol. 2017;36:39–47. [PubMed] [Google Scholar]
20. El-Sawalhi MM, Darwish HA, Mausouf MN, Shaheen AA. Modulation of age-related changes in oxidative stress markers and energy status in the rat heart and hippocampus: a significant role for ozone therapy. Cell Biochem Funct. 2013;31:518–525. [PubMed] [Google Scholar]
21. Cardile V, Jiang X, Russo A, Casella F, Renis M, Bindoni M. Effects of ozone on some biological activities of cells in vitro. Cell Biol Toxicol. 1995;11:11–21. [PubMed] [Google Scholar]
22. Gonzalez R, Borrego A, Zamora Z, et al. Reversion by ozone treatment of acute nephrotoxicity induced by cisplatin in rats. Mediators Inflamm. 2004;13:307–312. [PMC free article] [PubMed] [Google Scholar]
23. Valacchi G, Bocci V. Studies on the biological effects of ozone: 11. Release of factors from human endothelial cells. Mediators Inflamm. 2000;9:271–276. [PMC free article] [PubMed] [Google Scholar]
24. Re L, Martínez-Sánchez G, Bordicchia M, et al. Is ozone pre-conditioning effect linked to Nrf2/EpRE activation pathway in vivo. A preliminary result? Eur J Pharmacol. 2014;742:158–162. [PubMed] [Google Scholar]
25. Chang JD, Lu HS, Chang YF, Wang D. Ameliorative effect of ozone on cytokine production in mice injected with human rheumatoid arthritis synovial fibroblast cells. Rheumatol Int. 2005;26:142–151. [PubMed] [Google Scholar]
26. Madej P, Plewka A, Madej JA, et al. Ozonotherapy in an induced septic shock. I. Effect of ozonotherapy on rat organs in evaluation of free radical reactions and selected enzymatic systems. Inflammation. 2007;30:52–58. [PubMed] [Google Scholar]
27. Bocci VA, Zanardi I, Travagli V. Ozone acting on human blood yields a hormetic dose-response relationship. J Transl Med. 2011;9:66. [PMC free article] [PubMed] [Google Scholar]
28. Brigelius-Flohé R, Flohé L. Basic principles and emerging concepts in the redox control of transcription factors. Antioxid Redox Signal. 2011;15:2335–2381. [PMC free article] [PubMed] [Google Scholar]
29. Bocci V, Zanardi I, Huijberts MS, Travagli V. Diabetes and chronic oxidative stress. A perspective based on the possible usefulness of ozone therapy. Diabetes Metab Syndr. 2011;5:45–49. [PubMed] [Google Scholar]
30. León Fernández OS, Ajamieh HH, Berlanga J, et al. Ozone oxidative preconditioning is mediated by A1 adenosine receptors in a rat model of liver ischemia/reperfusion. Transpl Int. 2008;21:39–48. [PubMed] [Google Scholar]
31. Mancuso C. Bilirubin and brain: a pharmacological approach. Neuropharmacology. 2017;118:113–123. [PubMed] [Google Scholar]
32. Ajamieh HH, Menendez S, Martinez-Sanchez G, et al. Effects of ozone oxidative preconditioning on nitric oxide generation and cellular redox balance in a rat model of hepatic ischaemia-reperfusion. Liver Int. 2004;24:55–62. [PubMed] [Google Scholar]
33. Chen H, Xing B, Liu X, et al. Ozone oxidative preconditioning protects the rat kidney from reperfusion injury: the role of nitric oxide. J Surg Res. 2008;149:287–295. [PubMed] [Google Scholar]
34. Orakdogen M, Uslu S, Emon ST, Somay H, Meric ZC, Hakan T. The effect of ozone therapy on experimental vasospasm in the rat femoral artery. Turk Neurosurg. 2016;26:860–865. [PubMed] [Google Scholar]
35. Bocci V, Borrelli E, Travagli V, Zanardi I. The ozone paradox: ozone is a strong oxidant as well as a medical drug. Med Res Rev. 2009;29:646–682. [PubMed] [Google Scholar]
36. Gulmen S, Kurtoglu T, Meteoglu I, Kaya S, Okutan H. Ozone therapy as an adjunct to vancomycin enhances bacterial elimination in methicillin resistant Staphylococcus aureus mediastinitis. J Surg Res. 2013;185:64–69. [PubMed] [Google Scholar]
37. Bocci V. Does ozone really “cure” cancer. Int J Cancer. 2008;123:1222. author reply 1223. [PubMed] [Google Scholar]
38. Caliskan B, Guven A, Ozler M, et al. Ozone therapy prevents renal inflammation and fibrosis in a rat model of acute pyelonephritis. Scand J Clin Lab Invest. 2011;71:473–480. [PubMed] [Google Scholar]
39. Sweet F, Kao MS, Lee SC, Hagar WL, Sweet WE. Ozone selectively inhibits growth of human cancer cells. Science. 1980;209:931–933. [PubMed] [Google Scholar]
40. Hernández F, Menéndez S, Wong R. Decrease of blood cholesterol and stimulation of antioxidative response in cardiopathy patients treated with endovenous ozone therapy. Free Radic Biol Med. 1995;19:115–119. [PubMed] [Google Scholar]
41. Wainstein J, Feldbrin Z, Boaz M, Harman-Boehm I. Efficacy of ozone-oxygen therapy for the treatment of diabetic foot ulcers. Diabetes Technol Ther. 2011;13:1255–1260. [PubMed] [Google Scholar]
42. Martínez-Sánchez G, Al-Dalain SM, Menéndez S, et al. Therapeutic efficacy of ozone in patients with diabetic foot. Eur J Pharmacol. 2005;523:151–161. [PubMed] [Google Scholar]
43. Bertolotti A, Izzo A, Grigolato PG, Iabichella ML. The use of ozone therapy in Buruli ulcer had an excellent outcome. BMJ Case Rep. 2013;2013:bcr2012008249. [PMC free article] [PubMed] [Google Scholar]
44. Moore G, Griffith C, Peters A. Bactericidal properties of ozone and its potential application as a terminal disinfectant. J Food Prot. 2000;63:1100–1106. [PubMed] [Google Scholar]
45. Shah P, Shyam AK, Shah S. Adjuvant combined ozone therapy for extensive wound over tibia. Indian J Orthop. 2011;45:376–379. [PMC free article] [PubMed] [Google Scholar]
46. Tafil-Klawe M, Wozniak A, Drewa T, et al. Ozone therapy and the activity of selected lysosomal enzymes in blood serum of patients with lower limb ischaemia associated with obliterative atheromatosis. Med Sci Monit. 2002;8:CR520–525. [PubMed] [Google Scholar]
47. Romero Valdés A, Menéndez Cepero S, Gómez Moraleda M, Ley Pozo J. Ozone therapy in the advanced stages of arteriosclerosis obliterans. Angiologia. 1993;45:146–148. [PubMed] [Google Scholar]
48. Verrazzo G, Coppola L, Luongo C, et al. Hyperbaric oxygen, oxygen-ozone therapy, and rheologic parameters of blood in patients with peripheral occlusive arterial disease. Undersea Hyperb Med. 1995;22:17–22. [PubMed] [Google Scholar]
49. Giunta R, Coppola A, Luongo C, et al. Ozonized autohemotransfusion improves hemorheological parameters and oxygen delivery to tissues in patients with peripheral occlusive arterial disease. Ann Hematol. 2001;80:745–748. [PubMed] [Google Scholar]
50. Di Paolo N, Bocci V, Garosi G, et al. Extracorporeal blood oxygenation and ozonation (EBOO) in man. preliminary report. Int J Artif Organs. 2000;23:131–141. [PubMed] [Google Scholar]
51. Di Paolo N, Bocci V, Salvo DP, et al. Extracorporeal blood oxygenation and ozonation (EBOO): a controlled trial in patients with peripheral artery disease. Int J Artif Organs. 2005;28:1039–1050. [PubMed] [Google Scholar]
52. Molinari F, Rimini D, Liboni W, et al. Cerebrovascular pattern improved by ozone autohemotherapy: an entropy-based study on multiple sclerosis patients. Med Biol Eng Comput. 2017;55:1163–1175. [PubMed] [Google Scholar]
53. Molinari F, Simonetti V, Franzini M, et al. Ozone autohemotherapy induces long-term cerebral metabolic changes in multiple sclerosis patients. Int J Immunopathol Pharmacol. 2014;27:379–389. [PubMed] [Google Scholar]
54. Lintas G, Molinari F, Simonetti V, Franzini M, Liboni W. Time and time-frequency analysis of near-infrared signals for the assessment of ozone autohemotherapy long-term effects in multiple sclerosis. Conf Proc IEEE Eng Med Biol Soc. 2013;2013:6171–6174. [PubMed] [Google Scholar]
55. Clavo B, Santana-Rodriguez N, Gutierrez D, et al. Long-term improvement in refractory headache following ozone therapy. J Altern Complement Med. 2013;19:453–458. [PubMed] [Google Scholar]
56. Clavo B, Catalá L, Pérez JL, Rodríguez V, Robaina F. Ozone Therapy on Cerebral Blood Flow: A Preliminary Report. Evid Based Complement Alternat Med. 2004;1:315–319. [PMC free article] [PubMed] [Google Scholar]
57. Clavo B, Suarez G, Aguilar Y, et al. Brain ischemia and hypometabolism treated by ozone therapy. Forsch Komplementmed. 2011;18:283–287. [PubMed] [Google Scholar]
58. Bocci V, Travagli V, Zanardi I. Randomised, double-blinded, placebo-controlled, clinical trial of ozone therapy as treatment of sudden sensorineural hearing loss. J Laryngol Otol. 2009;123:820. author reply 820. [PubMed] [Google Scholar]
59. Ragab A, Shreef E, Behiry E, Zalat S, Noaman M. Randomised, double-blinded, placebo-controlled, clinical trial of ozone therapy as treatment of sudden sensorineural hearing loss. J Laryngol Otol. 2009;123:54–60. [PubMed] [Google Scholar]
60. Clavo B, Ruiz A, Lloret M, et al. Adjuvant ozonetherapy in advanced head and neck tumors: a comparative study. Evid Based Complement Alternat Med. 2004;1:321–325. [PMC free article] [PubMed] [Google Scholar]
61. Clavo B, Pérez JL, López L, et al. Ozone therapy for tumor oxygenation: a pilot study. Evid Based Complement Alternat Med. 2004;1:93–98. [PMC free article] [PubMed] [Google Scholar]
62. Menéndez S, Del Cerro A, Alvarez T, Hernández F. Application of ozone therapy in the vestibulocochlear syndrome. Rev Recent Clin Trials. 2012;7:321–328. [PubMed] [Google Scholar]
63. Borrelli E, Bocci V. Visual improvement following ozonetherapy in dry age related macular degeneration; a review. Med Hypothesis Discov Innov Ophthalmol. 2013;2:47–51. [PMC free article] [PubMed] [Google Scholar]
64. Steppan J, Meaders T, Muto M, Murphy KJ. A metaanalysis of the effectiveness and safety of ozone treatments for herniated lumbar discs. J Vasc Interv Radiol. 2010;21:534–548. [PubMed] [Google Scholar]
65. Paoloni M, Di Sante L, Cacchio A, et al. Intramuscular oxygen-ozone therapy in the treatment of acute back pain with lumbar disc herniation: a multicenter, randomized, double-blind, clinical trial of active and simulated lumbar paravertebral injection. Spine (Phila Pa 1976) 2009;34:1337–1344. [PubMed] [Google Scholar]
66. Oder B, Loewe M, Reisegger M, Lang W, Ilias W, Thurnher SA. CT-guided ozone/steroid therapy for the treatment of degenerative spinal disease--effect of age, gender, disc pathology and multi-segmental changes. Neuroradiology. 2008;50:777–785. [PubMed] [Google Scholar]
67. Magalhaes FN, Dotta L, Sasse A, Teixera MJ, Fonoff ET. Ozone therapy as a treatment for low back pain secondary to herniated disc: a systematic review and meta-analysis of randomized controlled trials. Pain Physician. 2012;15:E115–129. [PubMed] [Google Scholar]
68. Al-Jaziri AA, Mahmoodi SM. Painkilling effect of ozone-oxygen injection on spine and joint osteoarthritis. Saudi Med J. 2008;29:553–557. [PubMed] [Google Scholar]
69. Bonetti M, Fontana A, Albertini F. CT-guided oxygen-ozone treatment for first degree spondylolisthesis and spondylolysis. Acta Neurochir Suppl. 2005;92:87–92. [PubMed] [Google Scholar]
70. Bocci V, Paulesu L. Studies on the biological effects of ozone 1. Induction of interferon gamma on human leucocytes. Haematologica. 1990;75:510–515. [PubMed] [Google Scholar]
71. Zaky S, Kamel SE, Hassan MS, et al. Preliminary results of ozone therapy as a possible treatment for patients with chronic hepatitis C. J Altern Complement Med. 2011;17:259–263. [PubMed] [Google Scholar]
72. Zaky S, Fouad EA, Kotb HI. The effect of rectal ozone on the portal vein oxygenation and pharmacokinetics of propranolol in liver cirrhosis (a preliminary human study) Br J Clin Pharmacol. 2011;71:411–415. [PMC free article] [PubMed] []
73. Clavo B, Ceballos D, Gutierrez D, et al. Long-term control of refractory hemorrhagic radiation proctitis with ozone therapy. J Pain Symptom Manage. 2013;46:106–112. [PubMed] [Google Scholar]
74. Peretyagin SP, Vorobyov AV, Martusevich AK, et al. Ozonotherapy of the gastrointestinal tract stressinjuries at urgency patients and biocristalloscopic monitoring its effectiveness. Revista Ozonoterapia Rev. 2008;1:24–28. [Google Scholar]
75. Neimark AI, Nepomnyashchikh LM, Lushnikova EL, Bakarev MA, Abdullaev NA, Sizov KA. Microcirculation and structural reorganization of the bladder mucosa in chronic cystitis under conditions of ozone therapy. Bull Exp Biol Med. 2014;156:399–405. [PubMed] [Google Scholar]
76. Gu XB, Yang XJ, Zhu HY, Xu YQ, Liu XY. Effect of medical ozone therapy on renal blood flow and renal function of patients with chronic severe hepatitis. Chin Med J (Engl) 2010;123:2510–2513. [PubMed] [Google Scholar]
78. Bonforte G, Bellasi A, Riva H, et al. Ozone therapy: a potential adjunct approach to lower urinary tract infection? A case series report. G Ital Nefrol. 2013;30:gin/30.34.16. [PubMed] [Google Scholar]
Journal articleOpen Access
Medical ozone modifies D-dimer, interleukin-6, lactic acid and oxidative stress levels: A possibility for the comprehensive treatment of COVID-19
Ruíz-García, María Gema; De la Cruz-Enríquez, Joel; Rojas-Morales, Emmanuel; Martínez-Vásquez, Aldrín; Tobón-Velasco, Julio César; Vázquez-Reyes, Christian Javier; Jiménez-Ortega, José Carlos
ABSTRACT
Background: SARS-CoV-2-induced inflammation in COVID-19 is mediated by cytotoxic and pro-oxidant effects that potentiate alveolar, endothelial and immune tissue damage. Objective: We investigated the effect of medicinal ozone administration on the oxidative stress markers; in addition to D-dimer, lactic acid and interleukin-6 as markers of endothelial injury and inflammation process. Methodology: Medicinal ozone with oligo metals was administered in vivo (major autohemotherapy) and in vitro (peripheral blood), to subsequently determine the levels of: H2O2, NO, GPx, CAT, TAP, TBARs, D-dimer, lactic acid and interleukin-6. Results: Medicinal ozone administration with oligo metals induced changes in oxidative stress markers both in vitro and in vivo. The H2O2 and TBARs levels decreased, in turn, NO levels increased (cardiovascular function marker). On the other hand, the levels of the antioxidant enzymes (GPx and CAT) show slightly increase, which indicates an antioxidant enzyme system regulation that counteracts the pro-oxidative effect of the infection. Furthermore, interleukin-6 levels decreased indicating the regulation of the systemic inflammatory process. Finally, lactic acid and D-dimer levels were decreased, establishing an improvement of energy metabolism and endothelial function respectively. Conclusion: The medicinal ozone administration induce decrease in the markers levels of oxidative stress, inflammation and cellular damage, improving the enzymatic antioxidant capacity and cellular metabolism with decrease plaque aggregation that contribute to reducing the risk of vascular endothelial damage. These benefits could be feasible to integrate in the treatment of endothelial injury in COVID-19 patients.
Ozone Therapy Attenuates NF-κB-Mediated Local Inflammatory Response and Activation of Th17 Cells in Treatment for Psoriasis
1. Department of Dermatology, Third Xiangya Hospital, Central South University, Changsha, Hunan, China;
2. XiangYa School of Medicine, Central South University, Changsha, Hunan, China;
3. Department of Cell Biology and Anatomy, School of Medicine, and
4. Department of Biomedical Engineering, College of Engineering and Computing, University of South Carolina, Columbia, South Carolina
*These authors contributed equally to this work.
✉ Corresponding author: Jianyun Lu, Department of Dermatology, Third Xiangya Hospital, Central South University, No. 138 Tongzipo Rd, Changsha, Hunan 410013, China. Telephone: +86-731-88618936. Fax: +86-731-88618936. Email: [email protected]
Citation:
Zeng J, Lei L, Zeng Q, Yao Y, Wu Y, Li Q, Gao L, Du H, Xie Y, Huang J, Tan W, Lu J. Ozone Therapy Attenuates NF-κB-Mediated Local Inflammatory Response and Activation of Th17 Cells in Treatment for Psoriasis. Int J Biol Sci 2020; 16(11):1833-1845. doi:10.7150/ijbs.41940. https://www.ijbs.com/v16p1833.htm
Ozone therapy has been widely used to treat many skin diseases, including infections, allergic dermatosis, and skin ulcers. However, its efficacy as a treatment for psoriasis is unclear. In this study, we explored the clinical efficacy and the underlying molecular mechanisms of ozone therapy on psoriasis. We found that topical ozone treatment significantly decreased patients' psoriasis area and severity index (PASI) scores and the expression of psoriasis-associated cytokines in their peripheral blood CD4+ T cells. In the IMQ-induced psoriasis mouse model, topical ozone treatment significantly inhibited the formation of IMQ-induced psoriasis-like lesions and the expression of psoriasis-associated inflammatory factors. High-throughput sequencing confirmed that IMQ-induced activation of toll-like receptor 2 (TLR2)/ nuclear factor-κB (NF-κB) signaling pathway was significantly suppressed in psoriasis-like lesions after topical ozone treatment. Furthermore, the activation of spleen T helper (Th) 17 cells was blocked in the mouse model; this was associated with the downregulation of cytokines and NF-κB pathways upon topical ozone treatment. Ozone therapy can attenuate local inflammatory reactions and the activation of Th17 cells in psoriasis by inhibiting the NF-κB pathway. Our results show that ozone therapy is effective in treating psoriasis. We recommend further evaluations for its clinical applications.
Psoriasis vulgaris is a long-lasting immune-mediated inflammatory cutaneous disease that is characterized by red, itchy, and scaly skin patches. Patients generally suffer disfiguration, disability, and associated comorbidities [1]. Environmental risk factors, such as microbial infections, obesity, and exposure to ultraviolet radiation, can trigger the onset of the disease in patients with latent psoriatic genetic susceptibility [2]. Plasmacytoid dendritic cells (pDCs) have been identified as inducers in the inflammatory cascade in psoriatic plaques [3]. Local pDCs in psoriatic skin lesions can activate and induce the differentiation of T helper (Th) cells into Th17, Th1, and Th22 subsets by producing IL-23, IL-12, IL-6, and tumor necrosis factor (TNF)-α [4, 5]. Evidence has shown that proportions of Th1 and Th17 cells in the skin lesions and peripheral blood of psoriatic patients are significantly increased as compared with normal subjects; Th2 cells and their associated cytokines; including IL-4, IL-10, and IL-13, show decreased proportions [6, 7]. Therefore, the blocking of pathogenic T cell activation, particularly the Th17 subset, has led to many remedies, such as assecukinumab [8], ixekizumab [9], and brodalumab [10]. However, problems related to biological agents, such as the single effect, high costs, and drug resistance, are major concerns to many patients and physicians. In addition, multiple inflammatory cytokine-stimulated NF-κB pathways are constitutively activated in psoriatic epidermis, resulting in hyperproliferation of keratinocytes [11, 12]. Activation of toll-like receptor 2 (TLR2) in keratinocytes can lead to the nuclear translocation of NF-κB and release of the proinflammatory cytokines TNF-α and IL-8 [13]. Microorganisms and their components and pathogen-associated molecular patterns (PAMPs) can trigger TLR2 to induce immune system activation [14]. Therefore, targeting the TLR2/NF-κB pathway is a potential novel therapeutic strategy.
Ozone was first applied clinically as a sterilizing agent due to its strong oxidizing property. It has been widely used to treat more than 50 different pathological conditions, including infectious skin diseases [15-18], allergic diseases [19, 20], erythema scaly diseases [21, 22], wound healing, and ulcer recovery [23]. The mechanisms of ozone's action may underlie antimicrobial effects, immunoregulation, antioxidant defenses, epigenetic modification, biosynthesis, analgesics, and vasodilation [24]. Current ozone medical preparations for dermatology fall into the following primary classifications: ozone hydrotherapy, topical ozonated oil, ozone autohemotherapy (OAHT), and ozone gas cavity/acupoint injection [24]. Recent studies have shown that a precise control of ozone concentrations can induce the production of various cytokines, such as IFN-γ, IL-6, and TNF-α [25]. Ozone can induce and activate the body's antioxidant enzyme system to produce free radical scavenging agents, remove some of the free radicals generated by inflammatory reactions, and interfere with the production of inflammatory factors during disease development [26]. However, the exact mechanisms of ozone therapy in treating diseases need to be further elucidated.
In this study, we evaluated the therapeutic efficacy of a short-term ozone treatment for psoriatic patients. We investigated potential mechanisms of topical ozone therapy for psoriasis using the imiquimod- (IMQ) induced psoriasis-like mouse model. We found that ozone therapy attenuated inflammatory responses in psoriasis by inhibiting the NF-κB pathway. Our results show that ozone therapy is a safe and effective treatment for psoriasis and is worthy of further clinical evaluations and applications.
Materials and Methods
Patients
This study was approved by the institutional review board (IRB) of the Third Xiangya Hospital, Central South University, Changsha, Hunan, China. A total of 10 psoriatic patients diagnosed with psoriasis vulgaris were enrolled in the study, and written consent forms were signed by all subjects. Clinical information on the patients is shown in Supplementary Table 1. PASI scores were used to assess disease activity. Study inclusion criteria were for patients between the ages of 18 and 60 years old and with psoriasis vulgaris diagnosed by pathologic examinations. Exclusion criteria included being allergic to ozonated water or oil; pregnancy or breastfeeding; severe systemic diseases; and having received corticosteroids, vitamin D3 derivatives, immune inhibitors, biological therapy, or oral retinoids within the previous 2 weeks.
Mice
The BALB/c mice were purchased from Hunan SJA Laboratory Animal Co., Ltd. At the age of 6 weeks, female mice were all adaptively fed for 1 week and used for all experiments. All animals were raised and handled in the animal experiment center of Central South University in strict accordance with relevant laws and institutional guidelines. All animal procedures were approved and supervised by the Medicine Animal Care and Use Committee of the Third Xiangya Hospital of Central South University.
Topical Ozone Therapy
All participants were treated with an ozonated water shower (3.0±1.5 mg/L, HZ-2601B, Hunan Health Care Technology, Changsha, China) for 15 minutes, once per day, then treated with topical ozonated oil (20160522, with an approximate peroxide value of 2,000-2,400 mmol-equivalent/kg, Hunan Health Care Technology, Changsha, China) twice per day, for 14 days.
Evaluation of Clinical Photographs and Reflectance Confocal Microscope Images of Skin Lesions
All subjects received free ozone therapy only; they did not receive any other treatments and drugs during the trial. The intervention lasted 14 days. Clinical photographs, PASI scores, and RCM images were assessed by the same professional physicians in order to score disease severity before and after treatments. PASI scores included the area of skin lesions, erythema, scaling, and thickening, according to the literature [27]. Each subject was assessed by RCM images from three different skin lesion sites. The total RCM scanned thickness of the skin was 51 layers × 3.05 µm (vertically) in each layer. Under RCM, epidermal thickness and infiltrated inflammatory cells were also evaluated prior to and post-treatment.
IMQ-Induced Mouse Model of Psoriasis and Ozone Intervention
Female BALB/c mice (aged 6-8 weeks) were fed under suitable conditions. The mice were smeared daily with a topical 5% IMQ cream (Sichuan Med-Shine Pharmaceutical Co., Ltd., H20030128, Sichuan, China) on their shaved dorsal skins for 7 consecutive days. Mice in the control group were treated with the same quantity of the vehicle cream. All IMQ mice were randomly divided into three groups: the nonintervention group (IMQ group), the ozone-treatment group (IMQ+Ozone), and the vehicle cream-treatment group (IMQ+Vehicle). The ozone-treatment group was treated with ozonated water (HZ-2601B, Hunan Health Care Technology Co., Ltd., Changsha, China) for 15 minutes once per day, then treated with topical ozonated oil (20160522, Hunan Health Care Technology Co., Ltd., Changsha, China). The vehicle cream-treatment group received tap water and base oil at the same frequency. The intervention lasted for 7 days. Clinical photographs and PASI scores were collected in order to evaluate the phenotypic characteristics. At the 7th day, all mice were sacrificed to collect skin lesions, spleen tissues, and lymph nodes.
Isolation of CD4+ T Cells
Peripheral blood mononuclear cells (PBMCs) were separated from peripheral blood of patients before and after treatment by centrifugation using a density gradient medium (GE Healthcare, Chicago, IL, USA). CD4+ T cells were isolated by a positive selection using Miltenyi beads according to the manufacturer's instructions (Miltenyi Biotec, Bergisch Gladbach, Germany). Next, the isolated CD4+ T cells were collected for subsequent experiments. In the mouse experiment, CD4+ T cells were purified from pooled single-cell suspensions of spleen using a mouse CD4+ T cell isolation kit from Miltenyi Biotec (Bergisch Gladbach, Germany).
Flow Cytometry
Surface markers, cytokines, and transcriptional factors were detected using an FACSCanto II cell analyzer (BD Biosciences, San Jose, CA, USA). For cytokine detection, isolated cells were stimulated in vitro for 4 h with phorbol 12-myristate 13-acetate (PMA) and ionomycin (Sigma-Aldrich, St. Louis, MO, USA) with the addition of GolgiPlug (BD Biosciences, San Jose, CA, USA) to promote the release of cytokines. Subsequently, the treated cells were incubated with antibodies against surface markers on ice for 30 min in the dark. For intracellular staining, cells were fixed and permeabilized with an eBioscience forkhead box P3 (FOXP3) transcription factor staining buffer set (catalog No. 00-5523, San Diego, CA, USA) and then stained with fluorescent antibodies for an additional 30 min on ice in the dark. Items were collected and analyzed using the FlowJo software (FlowJo LLC, Ashland, OR, USA). The following antibodies were obtained from BioLegend (San Diego, CA, USA) and used in this study: FITC anti-mouse IFN-γ (catalog No. 505805), Alexa Fluor 647 anti-mouse IL-17A (catalog No. 506911), PE anti-mouse IL-4 (catalog No. 504103), PE anti-mouse FOXP3 (catalog No. 126403), PerCP/Cy5.5 anti-mouse CD4 (catalog No. 100540), and FITC anti-mouse CD3 (catalog No. 5100203). Phycoerythrin (PE) anti-mouse IL-4 was obtained from BD Biosciences (catalog No. 504103, San Jose, CA, USA) and APC anti-mouse CD25 was obtained from eBioscience (catalog No. 102011, San Diego, CA, USA).
qPCR
Total RNA was extracted from cells or skin tissues using TRIzol according to the manufacturer's instructions (Thermo Fisher Scientific, Waltham, MA, USA). The mRNA was reverse-transcribed with the PrimeScript® RT reagent kit (Takara Biomedical Technology Co., Ltd., Kusatsu, Shiga, Japan) with 1 μg of total RNA in each reaction. The reaction mixture for real-time PCR contained 2 μL of cDNA, 10 μL of SYBR Premix Ex Taq™ (Takara Biomedical Technology Co., Ltd., Kusatsu, Shiga, Japan), and 400 nM of sense and antisense primers for a final volume of 20 μL. The qPCR was performed on a LightCycler® 96 (Roche, Rotkreuz, Switzerland) thermocycler. The quantity of gene expression was calculated using the 2-ΔCt methods and normalized to glyceraldehyde-3-phosphate dehydrogenase (GAPDH). Primers are shown in Supplementary Table 2.
Western Blotting
CD4+ T cells were lysated and proteins were extracted using a nuclear extraction reagent (Boster Biological Technology, Pleasanton, CA, USA). Proteins were quantified by the Bradford reagent (Thermo Fisher Scientific, Waltham, MA, USA), followed by 12% vertical dodecyl sulfate-polyacrylamide gel electrophoresis. Proteins were then transferred into a polyvinylidene difluoride (PVDF) membrane (Sigma-Aldrich, St. Louis, MO, USA). The PVDF membrane was blocked in 5% skim milk for 1 h at room temperature, then incubated with an antibody against P65 (GB11142, 1:1000, Wuhan Servicebio Technology Co., Ltd., Wuhan, China) or P50 (ab7971, 1:5000, Abcam, Cambridge, MA, USA) for 12-16 h at 4℃ , and followed by incubating with a mouse anti-rabbit IgG antibody (H&L) (GenScript, Piscataway, NJ, USA). Proteins were detected with an enhanced chemiluminescence (ECL) western blot detection kit (Thermo Fisher Scientific, Waltham, MA, USA). Quantification of P65 and P50 was normalized to GAPDH by densitometry.
Histological Analysis
Skin tissues from all patients and mice were fixed in formalin and embedded in paraffin (Wuhan Servicebio Technology Co., Ltd., Wuhan, China). Sections (6 µm) were stained with hematoxylin and eosin and stored at room temperature. Epidermal thickness and infiltrating inflammatory cells were assessed.
Immunohistochemical Staining
Sections (6 µm) were stained with P50 (catalog No. BS1249, Bioworld Technology Co., Ltd., Nanjing, China), P65 (catalog No. 10745-1-AP, Proteintech, Rosemont, IL, USA) and TLR2 antibodies (catalog No. ab213676, Abcam, Cambridge, MA, USA) according to the manufacturers' instructions. Image analysis was performed using a fluorescent microscope and Leica Qwin Std analysis software (Leica, Wetzlar, Germany).
High-Throughput Sequencing
Transcriptome profiles of the left and right sides of the skin lesions from self-control mouse models and lesions from the mouse dorsal skins in the control group and the IMQ group were obtained. Briefly, total RNA was extracted from these skin samples; the mRNA was enriched, fragmented and used for the cDNA synthesis. The cDNA fragments were amplified by PCR, and the size and quality of sequencing library were determined using an Agilent 2100 Bioanalyzer (Agilent, Santa Clara, CA, USA). The library was sequenced using a HiSeq X Ten high-throughput sequencing platform (Illumina Inc., San Diego, CA, USA). The differentially expressed genes among the selected samples were analyzed by Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analysis.
Statistical Analysis
All of the diagrams and graphs reporting cumulative data were generated using a GraphPad Prism 6.0 (GraphPad Software, San Diego, CA, USA). The data are represented as means ± standard error of the mean (SEM). Distributions of the means were analyzed with nonparametric tests (SPSS 18.0, IBM, Armonk, NY, USA). Differences in individual treatments were analyzed by paired t tests. Statistical significance (*P < 0.05, **P < 0.01, ***P < 0.001) was assessed using a 2-tailed unpaired Student t test for comparisons between 2 groups and 1-way analysis of variance (ANOVA) with relevant post hoc tests for multiple comparisons.
Results
Topical ozone treatment improves the condition of skin lesions in psoriasis
In order to evaluate the efficacy of ozone therapy on psoriasis, we enrolled ten patients with a diagnosis of psoriasis via cutaneous histopathology in this study. Each patient's psoriatic condition was determined using a psoriasis area and severity index (PASI) score, which was assessed four times over two weeks. In addition, clinical photographs, reflectance confocal microscopy (RCM), and hematoxylin and eosin (HE) staining were used to evaluate each patient's pathological characteristics before and after treatment. The patients' psoriatic skin lesions improved significantly after ozone therapy; clinical and histological improvements were evident in patients (Figure 1a and b). There were obvious attenuations of inflammatory erythema and scales showing in clinical photographs (Figure 1a). Histology and RCM images showed that the epidermis was significantly thinner and that infiltrating inflammatory cells had decreased after 14 days ozone treatment as compared to before treatment (Figure 1b-d). Correspondingly, the PASI scores dropped significantly after the 14-day treatment as compared with baselines (Figure 1e). In order to investigate the potential mechanisms of ozone action on psoriasis, we assessed the expression levels of common psoriatic-associated cytokines and transcription factors in CD4+ T cells from the patients' peripheral blood using quantitative real-time PCR (qPCR). Being expected, the expression levels of IL-17a, IL-6, TNF-α, transforming growth factor (TGF)-β, IFN-γ, and NF-κB were down-regulated after ozone-treatment as compared with prior to treatment (Figure 1f). The expression levels of IL-17f and the Th17-cell-specific transcription factor retinoid-related orphan nuclear receptor c (RORc) decreased after ozone treatment, but the decrease had no statistical significance (Figure 1f). The expression of IL-10 increased after ozone treatment, but not significantly. These results were consistent with the clinical efficacy. Taken together, our results demonstrate that topical ozone treatment can improve the condition of psoriatic skin lesions in patients by an inhibition of inflammatory processes.
Figure 1Topical ozone treatment improves the pathological conditions of psoriatic skin lesions. (a) Clinical photographs of a psoriatic skin lesion on days 0 (D0) and 14 (D14) with an ozone therapy. (b) HE staining of psoriatic skin lesion before and after treatment. (c) Evaluation of RCM images showing the 25th and 50th scanning layers before and after treatment. (d) Statistical analysis of vertical swept layers of quantitative RCM images for an assessment of thickness of epidermis; (e) PASI scores for all participants. (f) Quantitative PCR to detect expression levels of cytokines and transcriptional factors in CD4+ T cells from peripheral blood of psoriasis patients before and after treatment. Note: * = P < 0.05; ** = P < 0.01; *** = P < 0.001; NS = no statistical significance.
Inhibition of IMQ-induced psoriasis-like phenotypes by topical ozone treatment
In order to further evaluate the therapeutic efficacy of topical ozone on psoriasis, we used IMQ to induce psoriasis-like lesions on dorsal skins of BALB/c mice [28]. Daily application of topical ozone resulted in a significant inhibition of IMQ-induced psoriasis-like lesions as compared to the vehicle-treatment group (water + base oil) (Figure 2a). The topical ozone treatment prevented IMQ-induced weight loss (Figure 2b) and improved PASI scores (Figure 2c) in the IMQ-induced psoriatic mice. Previous studies [6] have shown that IMQ can cause enlargement of the spleen in this mouse model. We found that topical ozone treatment resulted in a significant inhibition of the increased spleen-to-body-weight ratio as compared with the no-treatment or vehicle-treatment groups (Figure 2d). These results demonstrate that topical ozone treatment can inhibit IMQ-induced psoriasis-like phenotypes in this mouse model.
Inhibition of IMQ-induced psoriasis-like inflammation by topical ozone treatment
In order to further investigate the mechanism underlying topical ozone treatment for IMQ-induced psoriasis-like lesions, we treated the right side of each lesion with topical ozone and kept the left side of the lesion untreated as a contralateral control (Figure 3a). We analyzed transcriptomes in the skin lesions after ozone treatment by RNA sequencing (RNA-seq) and compared with the skin lesions without treatment. We found that IMQ caused an increase in expression of 3083 genes and decrease in expression of 2854 genes, respectively, as compared with the control (Figure 3b). KEGG pathway enrichment analysis revealed that the inflammatory-related signaling pathways such as NF-κB, TLR, TNF, and IL-17 were significantly activated in the IMQ-induced psoriasis mouse model (Figure 3c). In contrast, topical ozone treatment (right side of the lesion) increased expression levels of 1023 genes and decreased expression levels of 1000 genes, respectively, as compared to the lesions without treatment (the left side of the lesions) (Figure 3d). Interestingly, IMQ-induced activation of NF-κB, TLR, TNF, and IL-17 signaling pathways was significantly inhibited by topical ozone application (Figure 3e). Further quantitative RT-PCR confirmed that topical ozone therapy could significantly inhibit the expression of many chemokines, such as C-X-C motif ligand (CXCL) 1, CXCL2, and CXCL3, and psoriasis-associated inflammatory factors, including IL-17a, IL-17c, IL-17f, IL-1β, IL-8, IL-22, TNF-α, vascular endothelial growth factor (VEGF), defensin B14, S100A7, S100A8, and S100A9 (Figure 3f). These results demonstrate that topical ozone therapy can treat psoriasis lesions via inhibition of the local inflammatory processes.
Inhibition of TLR2/NF-κB signaling by topical ozone treatment
Many studies have shown that the TLR2/NF-κB signaling pathway promotes the release of multiple inflammatory factors in psoriasis lesions, aggravating the inflammatory response of psoriasis lesions. In order to examine whether topical ozone could inhibit TLR2/NF-κB signaling, we used immunohistochemistry to characterize the expression profiles of TLR2, P50, and P65 in IMQ-induced psoriasis-like lesions and in patients. We found that topical ozone treatment significantly decreased the IMQ-induced expression levels of TLR2, P50, and P65 in the mouse model (Figure 4a and b) and in patients with psoriasis (Figure 4c). Therefore, topical ozone treatment can significantly inhibit TLR2/NF-κB signaling in psoriatic skin lesions.
Suppression of Th17 differentiation by topical ozone treatment
Immune imbalance of CD4+ T subset is considered to be a critical factor in the pathogenesis of psoriasis. Evidence has shown that the PASI scores of psoriasis patients are positively related to IL-17 levels in serum and that Th17 cells are the main infiltrating T subset in psoriatic skin lesions [29]. Not surprising, ozone therapy resulted in a significant suppression of the IMQ-induced polarized Th17-cell proportions (Figure 5a and b). Ozone treatment significantly inhibited expression levels of T helper lymphocyte-associated cytokines (Figure 5c), including IL-17a, IL-17f, IL-10, and IFN-γ, and key transcription factors (Figure 5d), such as signal transducer and activator of transcription (STAT) 3, RORc, and NF-κB. Ultimately, we examined the expression levels of P50 and P65 in splenic CD4+ T cells among the four groups using western blotting. We found that ozone treatment significantly inhibited the expression of NF-κB (Figure 5e and f). Therefore, topical ozone therapy may suppress the IMQ-induced activation of RORc and NF-κB signaling pathways to regulate the differentiation of Th17 cells. Moreover, we also assessed the differentiated proportions of Th1 cells, Th2 cells, and regulatory T (Treg) cells. There was no significant effect on the levels of Th1 and Th2 cells; the proportion of Treg cells was upregulated slightly (Supplementary Figure 1a-c). These data demonstrate that ozone may act on psoriasis mainly by inhibiting the activation and proliferation of Th17 cells and expression of their associated cytokines.
Figure 2Topical ozone treatment significantly inhibits IMQ-induced psoriasis-like lesions in mouse skin. Mice were randomly divided into four groups: Ctrl, IMQ, IMQ+Vehicle, and IMQ+Ozone. (a) The skin lesions and histological features among different treatment groups. (b) Changes of body weight and (c) PASI scores for mice in different treatment groups. (d) Spleen and spleen-to-body-weight ratio in different treatment groups. Note: * = P < 0.05; ** = P < 0.01; *** = P < 0.001; NS = no statistical significance.
Figure 3Topical ozone treatment significantly inhibits IMQ-induced psoriasis- like inflammation. (a) Psoriasis-like lesions were induced on dorsal skins of mice using IMQ. Topical ozone cream was applied on the right side of the lesion but not on the left side of the lesion. (b) Transcriptome analysis showing that IMQ induced an upregulation and downregulation of expression levels of 3063 and 2854 genes, respectively, in lesions as compared with normal skin. (c) Enrichment of the upregulated KEGG signaling pathway in the IMQ group versus control group. (d) Transcriptome analysis showing that ozone treatment caused an upregulation and downregulation of expression levels of 1203 and 1000 genes, respectively, in lesions as compared with IMQ induction group in the self-control experiment. (e) Enrichment of downregulated KEGG signaling pathway in the IMQ+Ozone group versus IMQ group. (f) Validation of changes in various psoriasis-associated inflammatory factors using qPCR. Note: * = P < 0.05; ** = P < 0.01; *** = P < 0.001; NS = no statistical significance.
Figure 4Topical ozone treatment significantly inhibits TLR2/NF-κB signaling. (a) Expression levels of TLR2, P50, and P65 in skin lesions from Ctrl, IMQ, IMQ+Vehicle, and IMQ+Ozone groups were evaluated by immunohistochemical analysis. (b) Expression levels of TLR2, P50, and P65 in IMQ-induced self-control mouse skin lesions and (c) human psoriasis lesions before and after ozone treatment.
High concentrations of ozone can induce cell damage, leading to respiratory diseases, headaches, skin irritation, and so forth [30-32]. However, low concentrations of ozone in the therapeutic range (10-80 μg/ml of gas) can be effectively quenched by the body's powerful antioxidative capacity in order to avoid toxic effects on cells; such concentrations of ozone have been used as a sterilizing agent, promote wound healing, regulate immunity, and carried out analgesic functions [33]. Ozone can quickly produce oxygen, reactive oxygen species (ROS), lipid oxidation products (LOPs), and aldehydes when in contact with skin tissue. ROS function as short-acting messengers and quickly disappear; LOPs can enter the blood circulation through lymphatic vessels and capillaries, and function as long-acting messengers. Aldehydes combine with cysteine and glutathione (GSH) to form a stable olefin adduct that can enter various cells of the human body, activating the nuclear factor erythroid 2-related factor 2 (Nrf2)- antioxidant response element (ARE) signaling pathway to improve antioxidant capacity [33]. Ozone can play a therapeutic role in many inflammatory diseases due to its antioxidant capacity. For instance, ozone therapy ameliorates inflammation and endometrial injury in rats with pelvic inflammatory diseases [34]. Local ozone therapy inhibits the expression of inflammatory factors such as pentraxin-3 (PTX-3), IL-1β, and high-sensitivity C-reactive protein (Hs-CRP) in periodontitis patients [35]. We have shown that local ozone therapy not only can kill Staphylococcus aureus in atopic dermatitis but also can inhibit inflammation by inhibiting the expression of IL-4 [36, 37]. An increasing body of evidence suggests that ozone therapy may be able to replace or reduce clinical usages of antibiotics and glucocorticoids, thereby decreasing risks such as antibiotic resistance and side effects from the long-term use of glucocorticoids.
Figure 5Topical ozone treatment suppresses Th17 differentiation to mitigate psoriasis disease. (a) Flow cytometry to determine the proportion of Th17 cells in mouse spleens and lymph nodes from four groups, e.g. Ctrl, IMQ, IMQ+Vehicle, and IMQ+Ozone. (b) Statistical analysis of the proportion of Th17 cells among different groups. Quantitative PCR to examine expression levels of cytokines (c) and transcriptional factors (d) in CD4+ T cells isolated from mouse spleens and lymph nodes. Western blotting to evaluate expression levels of P65 (d) and P50 (e) in CD4+ T cells isolated from mouse spleens and lymph nodes from four groups. The relative expression levels were normalized to GAPDH levels. Note: * = P < 0.05; ** = P < 0.01; *** = P < 0.001; NS = no statistical significance.
Psoriasis is a chronic relapsing inflammatory skin disease. We posit that ozone therapy can control the progression of psoriasis by inhibiting the inflammatory response of skin lesions. Studies have found that ozonated oil not only delivers reactive oxygen but also maintains therapeutically active ozonated derivatives for a long time [38]. Our previous studies have found that ozonated oil is safe and effective for the treatment of stable psoriasis vulgaris, with an efficacy equivalent to that of intermediate-acting glucocorticoids [39]. In this study, we have demonstrated that patients' psoriatic skin lesions are mitigated significantly and that inflammatory biomarkers such as IL-17a, IL-6, TNF-α, TGF-β, and IFN-γ are downregulated significantly after ozone treatment. We have also shown that ozone therapy can significantly inhibit inflammatory-related pathways, such as NF-κB, TLR, TNF, and IL-17, in a psoriasis animal model. These data provide an insight into the mechanisms underlying the therapeutic effects of ozone therapy on psoriatic lesions.
Multiple studies have found elevated levels of TLRs in psoriatic lesions [40-43]. TLRs are a very important class of pattern recognition receptors (PRRs). After recognizing PAMPs, such as lipopolysaccharides, peptidoglycan, viral products, and bacterial nucleus components, TLRs activate downstream signaling pathways to induce innate immune activation by promoting the release of proinflammatory cytokines and initiating specific immune responses [44-46]. Abnormally increased PAMPs (such as lipopolysaccharides and peptidoglycan) in psoriatic lesions activate the NF-κB signaling pathway, promoting the expression of proinflammatory cytokines, which induces a strong inflammatory response in local psoriasis [47, 48]. In this study, we have shown that ozone treatment can significantly inhibit the TLR2/NF-κB signaling pathway in psoriatic lesions, thereby attenuating the local inflammatory response of psoriasis. There are a few potential explanations for this. First, ozone therapy can reduce the production of PAMPs by inhibiting colonized microorganisms on the surface of lesions, which reduces the activation of the TLR2/NF-κB pathway. Second, activation of the antioxidant system by ozone such as Nrf2-ARE in the body can antagonize the NF-κB-mediated inflammatory responses [49, 50]. Third, oxygen produced by ozone therapy can improve the hypoxic environment of psoriatic skin lesions and inhibit hypoxia-induced inflammatory responses.
The activation of Th17 cells is crucial for the inflammatory response of psoriasis vulgaris lesions [51]. Our results show that ozone treatment can significantly inhibit IMQ-induced increases in the number and active function of Th17 cells. Activation of the NF-κB signaling pathway can induce the activation of Th17 cells [52]. Therefore, ozone-mediated suppression of the activation of Th17 cells is probably due to the inhibition of NF-κB pathways. In addition to Th17 cells, other immune cells, such as Th1, Th2, dendritic cells (DCs), natural killer (NK) cells, and macrophages, are also involved in the inflammatory response of psoriasis [53]. However, our results show that ozone treatment has a minimal effect on these cells. Therefore, ozone likely has a specific effect on the regulation of Th17 cells during the treatment of psoriasis.
In addition to ozonated water and oil, ozone autohemotherapy and ozone gas cavity/acupoint injection have also been reported to improve the body's antioxidant capacity and regulate inflammation [54-56]. Whether these treatments can be used for psoriasis has yet to be determined. Ozone can also be used in combination with other agents in order to reduce side effects and increase efficacy. For example, combined intradiscal and periganglionic injection of medical ozone and steroids has a cumulative effect, leading to enhanced overall outcomes in the treatment of pain caused by disk herniation [57]. Local ozone therapy has a few side effects, such as irritating pain. It rarely produces systemic side effects. There are some limitations in this study. For example, there are no data regarding the long-term efficacy of the treatment or its impact on recurrence rates. The question of whether ozone treatment plays a regulatory role in the proliferation and differentiation of keratinocytes and in the vasodilation of psoriasis has not yet been answered.
This work was supported by the New Xiangya Talent Projects of the Third Xiangya Hospital of Central South University (Grant No. 20170309) and National Undergraduate Innovation Training Program of Central South University (Grant No. GS201910533570).
Competing Interests
The authors have declared that no competing interest exists.
References
1. Boehncke WH, Schon MP. Psoriasis. Lancet. 2015;386:983-94
2. Zeng J, Luo S, Huang Y, Lu Q. Critical role of environmental factors in the pathogenesis of psoriasis. The Journal of dermatology. 2017;44:863-72
3. Becher B, Pantelyushin S. Hiding under the skin: Interleukin-17-producing gammadelta T cells go under the skin?. Nature medicine. 2012;18:1748-50
4. Krueger JG. Hiding under the skin: A welcome surprise in psoriasis. Nature medicine. 2012;18:1750-1
5. Gutcher I, Becher B. APC-derived cytokines and T cell polarization in autoimmune inflammation. The Journal of clinical investigation. 2007;117:1119-27
6. Wu R, Zeng J, Yuan J, Deng X, Huang Y, Chen L. et al. MicroRNA-210 overexpression promotes psoriasis-like inflammation by inducing Th1 and Th17 cell differentiation. The Journal of clinical investigation. 2018;128:2551-68
7. Kagami S, Rizzo HL, Lee JJ, Koguchi Y, Blauvelt A. Circulating Th17, Th22, and Th1 cells are increased in psoriasis. The Journal of investigative dermatology. 2010;130:1373-83
8. Speeckaert R, van Geel N, Lambert J, Claeys L, Delanghe JR, Speeckaert MM. Secukinumab: IL-17A inhibition to treat psoriatic arthritis. Drugs of today (Barcelona, Spain: 1998). 2016;52:607-16
9. Toussirot E. Ixekizumab: an anti- IL-17A monoclonal antibody for the treatment of psoriatic arthritis. Expert opinion on biological therapy. 2018;18:101-7
10. Lebwohl MG, Papp KA, Marangell LB, Koo J, Blauvelt A, Gooderham M. et al. Psychiatric adverse events during treatment with brodalumab: Analysis of psoriasis clinical trials. Journal of the American Academy of Dermatology. 2018;78:81-9.e5
11. Yan S, Xu Z, Lou F, Zhang L, Ke F, Bai J. et al. NF-kappaB-induced microRNA-31 promotes epidermal hyperplasia by repressing protein phosphatase 6 in psoriasis. Nature communications. 2015;6:7652
12. Hara-Chikuma M, Satooka H, Watanabe S, Honda T, Miyachi Y, Watanabe T. et al. Aquaporin-3-mediated hydrogen peroxide transport is required for NF-kappaB signalling in keratinocytes and development of psoriasis. Nature communications. 2015;6:7454
13. Begon E, Michel L, Flageul B, Beaudoin I, Jean-Louis F, Bachelez H. et al. Expression, subcellular localization and cytokinic modulation of Toll-like receptors (TLRs) in normal human keratinocytes: TLR2 up-regulation in psoriatic skin. European journal of dermatology: EJD. 2007;17:497-506
14. Choudhary V, Uaratanawong R, Patel RR, Patel H, Bao W, Hartney B. et al. Phosphatidylglycerol Inhibits Toll-Like Receptor-Mediated Inflammation by Danger-Associated Molecular Patterns. The Journal of investigative dermatology. 2019;139:868-77
15. Bialoszewski D, Pietruczuk-Padzik A, Kalicinska A, Bocian E, Czajkowska M, Bukowska B. et al. Activity of ozonated water and ozone against Staphylococcus aureus and Pseudomonas aeruginosa biofilms. Medical science monitor: international medical journal of experimental and clinical research. 2011;17:Br339-44
16. Zanardi I, Burgassi S, Paccagnini E, Gentile M, Bocci V, Travagli V. What is the best strategy for enhancing the effects of topically applied ozonated oils in cutaneous infections?. BioMed research international. 2013;2013:702949
17. Ouf SA, Moussa TA, Abd-Elmegeed AM, Eltahlawy SR. Anti-fungal potential of ozone against some dermatophytes. Brazilian journal of microbiology: [publication of the Brazilian Society for Microbiology]. 2016;47:697-702
18. Jenerowicz D, Silny W, Danczak-Pazdrowska A, Polanska A, Osmola-Mankowska A, Olek-Hrab K. Environmental factors and allergic diseases. Annals of agricultural and environmental medicine: AAEM. 2012;19:475-81
19. Gershwin LJ. Comparative immunology of allergic responses. Annual review of animal biosciences. 2015;3:327-46
20. Di Paolo N, Gaggiotti E, Galli F. Extracorporeal blood oxygenation and ozonation: clinical and biological implications of ozone therapy. Redox report: communications in free radical research. 2005;10:121-30
21. Bocci V, Zanardia I, Valacchi G, Borrelli E, Travagli V. Validity of Oxygen-Ozone Therapy as Integrated Medication Form in Chronic Inflammatory Diseases. Cardiovascular & hematological disorders drug targets. 2015;15:127-38
22. Polydorou O, Halili A, Wittmer A, Pelz K, Hahn P. The antibacterial effect of gas ozone after 2 months of in vitro evaluation. Clinical oral investigations. 2012;16:545-50
23. Borges GA, Elias ST, da Silva SM, Magalhaes PO, Macedo SB, Ribeiro AP. et al. In vitro evaluation of wound healing and antimicrobial potential of ozone therapy. Journal of cranio-maxillo-facial surgery: official publication of the European Association for Cranio-Maxillo-Facial Surgery. 2017;45:364-70
24. Zeng J, Lu J. Mechanisms of action involved in ozone-therapy in skin diseases. International immunopharmacology. 2018;56:235-41
25. Wu D, Tan W, Zhang Q, Zhang X, Song H. Effects of ozone exposure mediated by BEAS-2B cells on T cells activation: a possible link between environment and asthma. Asian Pacific journal of allergy and immunology. 2014;32:25-33
26. Delgado-Roche L, Martinez-Sanchez G, Re L. Ozone oxidative preconditioning prevents atherosclerosis development in New Zealand White rabbits. Journal of cardiovascular pharmacology. 2013;61:160-5
27. Reich K, Gooderham M, Thaci D, Crowley JJ, Ryan C, Krueger JG. et al. Risankizumab compared with adalimumab in patients with moderate-to-severe plaque psoriasis (IMMvent): a randomised, double-blind, active-comparator-controlled phase 3 trial. Lancet. 2019;394:576-586
28. van der Fits L, Mourits S, Voerman JS, Kant M, Boon L, Laman JD. et al. Imiquimod-induced psoriasis-like skin inflammation in mice is mediated via the IL-23/IL-17 axis. Journal of immunology. 2009;182:5836-45
29. van der Fits L, Mourits S, Voerman JS, Kant M, Boon L, Laman JD. et al. Imiquimod-induced psoriasis-like skin inflammation in mice is mediated via the IL-23/IL-17 axis. Journal of immunology (Baltimore, Md: 1950). 2009;182:5836-45
30. English P, Balmes J. Associations between Ozone and Fine Particulate Matter and Respiratory Illness Found to Vary between Children and Adults. Implications for U.S. Air Quality Policy. American journal of respiratory and critical care medicine. 2019;199:817-9
31. Apte MG, Buchanan IS, Mendell MJ. Outdoor ozone and building-related symptoms in the BASE study. Indoor air. 2008;18:156-70
32. Balmes JR. Long-term Exposure to Ozone and Cardiopulmonary Mortality: Epidemiology Strikes Again. American journal of respiratory and critical care medicine. 2019;200:958-959
33. Bocci V, Di Paolo N. Oxygen-ozone therapy in medicine: an update. Blood purification. 2009;28:373-6
34. Wei A, Feng H, Jia XM, Tang H, Liao YY, Li BR. Ozone therapy ameliorates inflammation and endometrial injury in rats with pelvic inflammatory disease. Biomedicine & pharmacotherapy = Biomedecine & pharmacotherapie. 2018;107:1418-25
35. Tasdemir Z, Oskaybas MN, Alkan AB, Cakmak O. The effects of ozone therapy on periodontal therapy: A randomized placebo-controlled clinical trial. Oral diseases. 2019;25:1195-202
36. Qin G, Huang J, Pan Y, Xiang Y, Ou C, Huang J. et al. [Topical ozone application: An innovative therapy for infantile atopic dermatitis]. Zhong nan da xue xue bao Yi xue ban. 2018;43:163-7
37. Lu J, Li M, Huang J, Gao L, Pan Y, Fu Z. et al. [Effect of ozone on Staphylococcus aureus colonization in patients with atopic dermatitis]. Zhong nan da xue xue bao Yi xue ban. 2018;43:157-62
38. Travagli V, Zanardi I, Valacchi G, Bocci V. Ozone and ozonated oils in skin diseases: a review. Mediators of inflammation. 2010;2010:610418
39. Tan L, Huang J, Lu J, Lu J. [Clinical efficacy of ozonated oil in the treatment of psoriasis vulgaris]. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2018;43:173-8
40. Liu Y, Yin H, Zhao M, Lu Q. TLR2 and TLR4 in autoimmune diseases: a comprehensive review. Clinical reviews in allergy & immunology. 2014;47:136-47
41. Begon E, Michel L, Flageul B, Beaudoin I, Jean-Louis F, Bachelez H. et al. Expression, subcellular localization and cytokinic modulation of Toll-like receptors (TLRs) in normal human keratinocytes: TLR2 up-regulation in psoriatic skin. European journal of dermatology: EJD. 2007;17:497-506
42. Candia L, Marquez J, Hernandez C, Zea AH, Espinoza LR. Toll-like receptor-2 expression is upregulated in antigen-presenting cells from patients with psoriatic arthritis: a pathogenic role for innate immunity?. The Journal of rheumatology. 2007;34:374-9
43. Shao S, Fang H, Dang E, Xue K, Zhang J, Li B. et al. Neutrophil Extracellular Traps Promote Inflammatory Responses in Psoriasis via Activating Epidermal TLR4/IL-36R Crosstalk. Frontiers in immunology. 2019;10:746
44. Kay E, Scotland RS, Whiteford JR. Toll-like receptors: Role in inflammation and therapeutic potential. BioFactors (Oxford, England). 2014;40:284-94
45. Mahla RS, Reddy MC, Prasad DV, Kumar H. Sweeten PAMPs: Role of Sugar Complexed PAMPs in Innate Immunity and Vaccine Biology. Frontiers in immunology. 2013;4:248
46. Brown J, Wang H, Hajishengallis GN, Martin M. TLR-signaling networks: an integration of adaptor molecules, kinases, and cross-talk. Journal of dental research. 2011;90:417-27
47. Lee JH, Moon JH, Lee YJ, Park SY. SIRT1, a Class III Histone Deacetylase, Regulates LPS-Induced Inflammation in Human Keratinocytes and Mediates the Anti-Inflammatory Effects of Hinokitiol. The Journal of investigative dermatology. 2017;137:1257-66
48. Chen JQ, Szodoray P, Zeher M. Toll-Like Receptor Pathways in Autoimmune Diseases. Clinical reviews in allergy & immunology. 2016;50:1-17
49. Lu MC, Zhao J, Liu YT, Liu T, Tao MM, You QD. et al. CPUY192018, a potent inhibitor of the Keap1-Nrf2 protein-protein interaction, alleviates renal inflammation in mice by restricting oxidative stress and NF-κB activation. Redox biology. 2019;26:101266
50. Subedi L, Lee JH, Yumnam S, Ji E, Kim SY. Anti-Inflammatory Effect of Sulforaphane on LPS-Activated Microglia Potentially through JNK/AP-1/NF-κB Inhibition and Nrf2/HO-1 Activation. Cells. 2019;8:pii E194
51. Visvanathan S, Baum P, Vinisko R, Schmid R, Flack M, Lalovic B. et al. Psoriatic skin molecular and histopathologic profiles after treatment with risankizumab versus ustekinumab. The Journal of allergy and clinical immunology. 2019;143:2158-69
52. Zhou F, Zhu Z, Gao J, Yang C, Wen L, Liu L. et al. NFKB1 mediates Th1/Th17 activation in the pathogenesis of psoriasis. Cellular immunology. 2018;331:16-21
53. Deng Y, Chang C, Lu Q. The Inflammatory Response in Psoriasis: a Comprehensive Review. Clinical reviews in allergy & immunology. 2016;50:377-89
54. Sancak EB, Turkon H, Cukur S, Erimsah S, Akbas A, Gulpinar MT. et al. Major Ozonated Autohemotherapy Preconditioning Ameliorates Kidney Ischemia-Reperfusion Injury. Inflammation. 2016;39:209-17
55. Deng L, Meng W, Li D, Qiu D, Wang S, Liu H. The effect of ozone on hypoxia, hemolysis and morphological change of blood from patients with aortic dissection (AD): a preliminary experiment of ozonated autohemotherapy for treating AD. American journal of translational research. 2018;10:1829-40
56. Chen H, Yu B, Lu C, Lin Q. The effect of intra-articular injection of different concentrations of ozone on the level of TNF-α, TNF-R1, and TNF-R2 in rats with rheumatoid arthritis. Rheumatology international. 2013;33:1223-7
57. Andreula CF, Simonetti L, De Santis F, Agati R, Ricci R, Leonardi M. Minimally invasive oxygen-ozone therapy for lumbar disk herniation. AJNR American journal of neuroradiology. 2003;24:996-1000
Updated Review on Ozone Therapy in Pain Medicine
Francisco Javier Hidalgo-Tallón1*Luis Miguel Torres-Morera2Jose Baeza-Noci3Maria Dolores Carrillo-Izquierdo4Rosa Pinto-Bonilla3
1Institute of Neurosciences, University of Granada, Granada, Spain
2Department of Anesthesia, Resuscitation, and Pain Treatment Service, Hospital Puerta del Mar, Cadiz, Spain
3Department of Embryology and Human Anatomy, School of Medicine, University of Valencia, Valencia, Spain
4School of Nursing, Catholic University of Murcia (UCAM), Murcia, Spain
The use of medical ozone in the treatment of chronic pain is progressively expanding in Spain and today it is used both in public and private medical centers. However, there is a great lack of knowledge about this technology not only in primary care but also in medical specialties. Although its biochemical bases are well determined and there are various systematic reviews and meta-analyses in the literature that justify its use in pain medicine, some professionals still are prejudiced against it. The evidence level of using medical ozone according SIGN (Scotish Intercollegiate Guideline Network) criteria is similar or superior to most of the techniques used in a Pain Unit. In this paper, we have done a review on ozone therapy in pain medicine, compiling the evidence published about it.
Introduction
Ozone therapy is the use of medical ozone as a therapeutic substance in pathologies with chronic hypoxia, inflammation, and redox imbalance in which ozone has proven to be effective (Baeza et al., 2015). Medical ozone is a mixture of oxygen and ozone obtained from medical oxygen by using a medical device – a medical ozone generator approved by a Notified Body according to the European Directive 93/42 and national regulations (Spanish RD 1591/2009). Medical ozone generators for parenteral use are classified in heading IIB of the classification of medical devices in EU regulations. Ozone therapy in medicine is a growing reality, and there are more and more professionals using medical ozone as a therapeutic tool for different diseases related to chronic oxidative stress and inflammation, including chronic pain.
In addition to health professional associations (such as the Spanish Ozone Therapy Association—SEOT or the World Federation of Ozone Therapy—WFOT) that try to unify criteria and develop protocols of treatment, as well as training health professionals in the use of this substance, the Catholic University of Murcia has taken the initiative by creating a chair of Ozone Therapy and Chronic Pain to better promote training and researching inside the Spanish universities network.
In Portugal and Greece, ozone therapy has a specific regulation and is used in public and private centers. In the rest of the European Union, it is used thanks to the legal recognition of medical ozone generators. In 2011, the Spanish Ministry of Health included the ozone therapy in the portfolio of services of the pain units (Palanca-Sánchez et al., 2011), so it is necessary that doctors who are experts in pain management know the rationale of medical ozone therapy and how it works, both locally and systemically.
Ozone is a molecule composed of three oxygen atoms (O3) instead of the two oxygen atoms found in the oxygen molecule (O2). Ozone has a half-life of 40 min at 20°C (Baeza et al., 2015); for this reason, it cannot be stored and must be produced “in situ” for each application.
Medical ozone applications date back to the beginning of the last century. The papers compiled in this publication have been published in the last 25 years and the oldest one have been included for historic reasons. Dr. Kellogg, in his book on diphtheria (1881) already mentioned ozone as a disinfectant, and in 1898 Drs Thauerkauf and Luth founded in Berlin the “Institute for oxygen therapy,” carrying out the first trials with animals. In 1911, the book “A Working Manual of High-Frequency Currents”, published by Dr. Noble Eberhart, head of the department of physiological therapeutics at Loyola University, described the use of medical ozone in the treatment of diseases such as tuberculosis, anemia, asthma, bronchitis, hay fever, diabetes, etc. (Pressman, 2021). But despite the successes achieved at the beginning of the last century, the ozone generating machines lacked precision and were quite fragile as they used a lot of glass tubes.
When applying this therapy, we are really inducing a controlled and harmless “micro-oxidation” that will produce a modulation of the cellular antioxidant system and the inflammation system. Ozone reacts with interstitial fluids producing hydrogen peroxide (H2O2), aldehydes, and lipid oxidation products (LOPs). These substances induce activation of the nuclear factor erythroid 2-related factor 2 (NRF2) pathway that will induce an increase in antioxidant systems (ARE), such as superoxide dismutase (SOD), catalase (CAT), reduced glutathione (GSH), glutathione peroxidase (GSH-Px), glutathione s-tranferase (GSTr), hem-oxygenase-1 (HO-1), reduced nicotinamide adenine dinucleotide phosphate (NADPH), NADPH quinone oxidoreductase 1 (NQO1) and heat shock protein-70 (HSP70; Baeza et al., 2015). This NRF2 activation (Figure 1) induces a decrease in the nuclear factor kappa beta (NFKβ) pathway activity, inducing an anti-inflammatory effect [decrease of interleukynes 1,2,6,7 and tumor necrosis factor alpha (TNFα) and increase of interlukynes 4, 10, 13 and transforming growing factor beta (TGFβ)] In the injected tissues, medical ozone inactivates proteolytic enzymes through the inhibition of the NFKβ pathway. At the same time, there is a proliferation of fibroblasts and chondrocytes, favoring cartilaginous regeneration (Fernández-Cuadros et al., 2020).
figure 1
FIGURE 1. The chemical reaction between ozone and PUFA (poli-unsaturated fatty acids) in the insterstitial water (or plasma) produce several ROS, mainly H2O2, and several LOPs, mainly 4-HNE (4-hydroxynonenal). Almost all H2O2 is kidnaped by erythrocytes (not reflected in this figure) if present. In nucleated cells, LOPs activates the NRF2 pathway, inducing the production of ARE (antioxidant response elements) and blocking the NFKB pathway. A small amount of H2O2 stimulates the NFKB pahtway, usually balanced with the NRF2 blocking action, producing a inmmunomodulation.
Several authors have published preclinical studies on the effects of medical ozone on living organisms, being able to demonstrate beneficial effects on the ability to modulate the redox balance, the cellular inflammation status, and the adaptation to ischemia/reperfusion processes (Barber et al., 1998; Peralta et al., 2000; Ajamieh et al., 2003, 2004, 2005).
From a clinical point of view, ozone therapy presents multiple medical-surgical applications, all of them related to the germicidal capacity of ozone, chronic ischemic and inflammation processes, and imbalance of the cellular redox status. Several manuals collect the experience and scientific work carried out to date by different research groups, mainly Italians, Germans, Russians, and Cubans (Bocci, 2002; Menéndez et al., 2008).
The forms of application of medical ozone are basically three: topical, infiltrative, and systemic (Baeza et al., 2015). Topical applications take advantage of the germicidal power of ozone and its positive effect on the healing processes; it is usually applied directly, with the use of zip-lock bags, or by using ozonated water or ozonated oils. Infiltrated ozone at concentrations between 4 and 30 μg/ml is useful for treating musculoskeletal diseases such as arthritis, tendonitis, myositis, fasciitis, neuritis, or myofascial pain. Systemic ozone therapy consists of the administration of the mixture of gasses mainly through two routes: the indirect intravenous way (also known as autohemotherapy) and the rectal insufflation. Indirect intravenous administration consists of extracting a determined blood quantity that, within a closed circuit, is put into contact with the gas, which will dissolve and react in a few seconds, and immediately reinfused. Certified (EU marked) medical devices should be used for this procedure. Rectal insufflation consists of administering a gas enema with a probe into the rectum, where it reacts with rectal mucus and generates peroxides. These are absorbed by the mucosa, reaching the hemorrhoidal plexus and the general venous blood circulation system like any other rectal treatment. The probes must be made of silicone or other ozone-resistant plastic (OzoneSolution, 2021).
Infiltrations With Medical Ozone (O2/O3)
Generalities
The use of O2/O3 infiltrations to treat musculoskeletal pathology is increasingly widespreading. Verga (1989) was the first to describe ozone intramuscular applications at the paravertebral level and trigger points in patients with chronic low back pain. Later, in the 90s, this procedure was also used to treat acute and chronic polyarthritis (hip, knee, sacroiliac joint, and interphalangeal), tendinitis, epicondylitis, carpal tunnel syndrome, and myofascial pain (Ajamieh et al., 2005).
Despite its frequent use, the level of evidence in many of the mentioned indications, but for the treatment of lumbar disk herniation and knee osteoarthritis, is low, possibly because it has been mainly used for years in private practice where randomized clinical trials are difficult to carry out. Carmona (2005) published in 2005 a systematic review on the efficacy of ozone therapy in rheumatic diseases, concluding that there were no quality clinical trials, that most of the works were published in low-impact journals, and that the methodology between the different studies is highly variable. However, this situation is changing, as more countries are using medical ozone in public centers and universities.
Therapeutic Properties and Mechanisms of Action of Injected Ozone
When we infiltrate the oxygen/ozone mixture, we are infiltrating a highly oxidizing gas, with a good tissue diffusion capacity. Apart from the general biochemical effect described in the Introduction section, several authors have described the anti-inflammatory, analgesic, and anti-edema properties of injected medical ozone, and propose that the oxidation of the algogenic receptors would inhibit the pain signal and it would activate the antinociceptive system (Re et al., 2010). This fact has been checked in one preclinical study from Fuccio et al. (2009) by inducing sciatic damage in mice, He confirmed the corticofrontal activation of genes of caspase 1, 8, and 12 (pro-inflammatory, pro-apoptotic, and responsible for allodynia) caused by the injury; this expression was normalized with a single peripheral injection of O2/O3 around the damaged area, which also reduced mechanical allodynia.
These properties would favor a muscle relaxant effect, as well as improved mobility of the treated area that can be observed clinically (Siemsen, 1995). This fact is very important in muscle recovery with O2/O3 injections. Balkanyi (1989) has described the utility of ozone therapy in the treatment of painful muscle hypertonia, highlighting the tremendous muscle relaxant effect that is produced.
Regarding the nucleus pulposus of the intervertebral disk, several authors have described that ROS will react with amino acids and carbohydrates of proteoglycans and collagen I and II that make up the matrix, giving a lead to a process of “mummification” which would shrink the disk, reducing the compression (Hawkins and Davies, 1996; Bocci et al., 2001; Leonardi et al., 2001). Iliakis and his group studied the histological changes of the nucleus pulposus matrix after treatment with an ozone intradiscal injection at a concentration of 27 μg/ml in rabbits and humans (resected disk specimens using microdiscectomy after the failure of the ozone treatment). Five weeks after the injection there were no signs of perilesional chondrocytic hyperplasia or inflammatory infiltrates typically observed in herniated disks biopsies; there was a fibrous tissue of less volume (“disk mummified”), which supposes a decrease in compression on the nerve root, a decrease in venous ecstasy, an improvement in local circulation, greater oxygenation and less pain, given the great sensitivity to hypoxia of nerve roots (Iliakis et al., 2001). Similar findings in pigs at different ozone concentrations were reported by Muto (2004).
Dosage
Regarding dosage, standardized protocols are lacking. Most authors relate the amount of the gas mixture to the extension of the injury or to the size of the joint cavity to be infiltrated. Generally, the amounts of gas range between 5 and 15 ml, and ozone concentrations range from 4 to 30 μg/ml. The number of infiltration sessions usually ranges from 3 to 10 (usually one or two per week) depending on the specific evolution of each case. About intradiscal injection, 2 ml for cervical and 5 for ml is the most used amount. If a patient does not respond to treatment after two or three interventions (once every 2 weeks) it is considered a failure. Torres et al. (2009) in a 2009 publication, after having used different concentrations with the same clinical protocol, observed more improvements when intradiscal O2/O3 is infiltrated at 50 μg/ml compared to lower concentrations (25 and 30 μg/ml). Nevertheless, we recommend not reaching 50 μg/ml due to the risk of iatrogenic injuries on the ring that have been detected experimentally in pigs (Muto, 2004).
This lack of standardization in the treatment protocols makes difficult to compare results when performing a systematic review, not allowing to get high quality conclusions or recommendations.
Ozone Therapy in Knee Pathology
One of the historic references was done in 1989 by Riva (1989), that registered 156 patients with knee joint pathology (post-traumatic arthritis, knee osteoathritis with mild deformity, and knee osteoathritis with severe deformity) obtaining good results that were especially positive when there were no severe bone deformities. The treatment consisted of intra-articular and periarticular infiltrations of 10 ml of medical ozone at a concentration of 20 μg/ml.
Later, In Cuba, a prospective study was carried out in 1997 to evaluate the efficacy and safety of medical ozone injections in 126 patients with knee osteoarthritis; usually, three or four injections were needed to obtain positive results, and only 14 patients received more than five sessions. 71.4% of the patients had a good result, in 10.3% the result was fair, and in 18.3% the result was bad. The main complication was pain during infiltration. It was highlighted the economic savings due to the low cost of the infiltrations and the lesser need for anti-inflammatory drugs (Escarpanter et al., 1997). Several authors have also published their experience in case series (Delgado and Quesada, 2005; Huanqui et al., 2006) and even proposed a treatment guide for based on their personal experience (Gheza and Bissolotti, 2003).
Moretti et al. (2004a) worked on the early knee osteoarthritis, comparing intraarticular injected O2/O3 with intraarticular hyaluronic acid, concluding that although there were no statistically significant differences in efficacy, ozone could be more indicated in the early stages of this disease, where inflammation predominates. In the same line, Giombini et al. (2016) published a randomized control trial comparing three kinds of injections: medical ozone, hyaluronic acid, and the combination. This last group showed the best outcomes and the hyaluronic acid group was more effective than ozone but without statistically significant differences. A systematic review and meta-analysis from Li et al. (2018) comparing medical ozone and hyaluronic acid had similar results, checking that hyaluronic acid was better than ozone but both improved the clinical status of the patients and had no significant side effects. A publication from Lopes de Jesus et al. (2017) demonstrated through a multicenter randomized, double-blind clinical trial the efficacy of intra-articular ozone injections versus placebo in knee osteoarthritis. In 2018 (Anzolin and Bertol, 2018; Costa et al., 2018; Raeissadat et al., 2018), 2019 (Arias-Vázquez et al., 2019; Noori-Zadeh et al., 2019) and 2020 (Sconza et al., 2020), six systematic reviews and meta-analyses were published in different journals supporting the use of ozone in knee osteoarthritis with a high level of evidence (GRADE 1+; Table 1).
These studies do not compare the results according to the radiological status of the knee, and we think this is basic fact, because hyaluronic acid is not indicated for moderate or severe knee osteoarthritis. Further studies in this line are needed to clarify the indications for medical ozone. Cost-efficacy studies are also needed as medical ozone is far cheaper than hyaluronic acid.
Other inflammatory knee pathologies have also been studied. Peritendinosus injected ozone has been used with success in refractory knee tendinopathies (Gjonovich et al., 2003). They improved 36 athletes with “jumper’s knee” who had not improved after conventional treatments.
Patellofemoral chondromalacia is a painful pathology whose treatment is mainly surgical, after which there is often aftermath. Manzi and Raimondi (2002) treated 60 patients with injected O2/O3 that had persistent pain after conventional surgical treatment, obtaining a higher and faster resolution of the pain in the treatment group compared to the control group.
Ozone Therapy in Shoulder Pathology
Gjonovich et al. (2002) published a prospective controlled study of patients suffering from subacromial tendinopathy treated with injected ozone versus mesotherapy; the ozone group showed superior clinical results. Ikonomidis et al. (2002) demonstrated in a double-blind clinical trial the greater efficacy of injected O2/O3 versus steroid injections and physiotherapy also in subacromial tendinopathy.
Oxygen-ozone therapy has also been used successfully in combination with shock waves, to treat calcifying tendinitis of the shoulder (Trenti and Gheza, 2002). Brina and Villani (2004) have published the utility of ultrasound-guided O2/O3 infiltrations in patients with non-surgical lesions of the rotator cuff. Medical ozone can increase the efficacy of other substances, as it was shown in paper of Moretti (2011) with hyaluronic acid and in paper of Gurger et al. (2021) with platelet-rich plasma (PRP); this last paper verifies the collaborative effect of ozone and PRP from a histological point of view.
Ozone Therapy in Spinal Pathology
Undoubtedly, the largest number of published works focuses on the use of ozone therapy for the treatment of herniated disks, both cervical and lumbar.
The treatment of cervical herniated disks is generally more conservative than that of the lumbar, perhaps due to the higher index of serious complications from your surgery (Wang et al., 2007). In this context, the interest in intradiscal or paravertebral medical ozone injections has special relevance, and the analgesic, anti-inflammatory, and muscle relaxant effects of the ozone therapy in cervical pathology have been described (Albertini, 2002; Villa, 2002).
In 2004, Moretti et al. (2004b), conducted a clinical trial comparing the efficacy of ozone therapy versus mesotherapy in patients with neck pain, upper limb paresthesias (uni or bilateral), peripheral vertigo, and headache. One hundred and fifty two patients had hernias, protrusions, or spondylosis, 76 of which were treated with medical ozone infiltrations in paravertebral muscles, the trapezius, and the elevators of the scapula; the other 76 patients were treated with anti-inflammatory drugs and mesotherapy. The differences were statistically significant in favor of the group treated with oxygen-ozone with 78% of optimal or good results, compared to 56.25% in the group of mesotherapy.
Regarding cervical intradiscal injections, a work published by Xiao et al. (2006) also supports their efficacy. Eighty-six patients with cervical spondylosis treated with CT-guided infiltrations were retrospectively assessed. Thirty-seven suffered from myelopathy, 30 had radiculopathy and 19 had sympathetic symptoms. The indication for treatment was cervicalgia with neurological symptoms (brachial irradiation patterns, loss of tenderness, tingling, numbness, muscle weakness, or deficiency of deep tendon reflexes) and all should be refractory to conservative therapies for at least 12 weeks. Patients with cervical spinal stenosis, ossification of the posterior longitudinal ligament were excluded. The treatment with ozone therapy was excellent, good, or poor in 78, 16, and 6% of the cases, respectively, as recorded with the modified MacNab Scale. These results coincide with those published by Alexandre et al. (2005) in the same year.
In lumbar pathology the number of published works is large. The good results, along with the safety of the technique and the dreaded complications of the surgery, have made more and more authors consider ozone therapy, either paravertebral or intradiscal, the first choice in case of failure of conservative treatment.
Andreula et al. (2003) added intradiscal and periganglionic O2/O3 to the infiltration with local anesthetics and steroids; in the 6 months follow-up, by blind evaluators, a statistically significant improvement was observed with the combination of both treatments. No side effect was detected. Buric et al. (2003) did a prospective follow-up over 18 months of 104 patients with lumbosciatic pain due to disk protrusions treated with intradiscal and intraforaminal O2/O3 injections, finding improvements in pain and functional capacity in most of them. Disk volume measurements were made with MRI and it was observed that, at 5 months, 22% of the protrusions had not changed in volume, 41% had reduced the size and 37% had disappeared. The results indicated that the technique was effective in the treatment of protrusions, although the efficacy was not higher than that of the microdiscectomy, according to the authors’ experience (Buric, 2005). Also regarding disk protrusions, Qing et al. (2005), in a sample of 602 patients and 1,078 operated disks, concluded the suitability treatment with ozone therapy as the first choice after failure more conservative techniques. When comparing ozone therapy with other minimally invasive techniques, these authors considered that it was an effective, safe, and minimally stressful technique for the patient and easy to perform.
Bonetti et al. (2005), in a randomized clinical trial, compared the efficacy of intraforaminal infiltration of O2/O3 with periradicular infiltration of steroids. Three hundred and six patients with low back pain and neuropathic leg pain with and without disk disease (spondylosis, spondylolisthesis, and facet joint degeneration) were recruited and randomly divided into two groups (166 and 140). The main measuring instrument was the modified MacNab scale. Patients were evaluated in the short (1 week), medium (3 months), and long term (6 months). In short term, there were no statistically significant differences between the two treatment modalities (p = 0.4077). In long term, the differences in favor of ozone treatments were statistically significant, but only in the group of patients with disk disease (p = 0.0021); also in long term, it could be seen that ozone therapy treatments had statistically lower failure rate (8.6%) than treatments with steroids (21.4%).
Muto et al. (2008) performed CT-guided injections to 2,900 patients with lumbosciatic pain due to herniated disks (including relapses). The gas was injected intradiscal, peri-ganglionic, and periradicular. After a month the patients were reviewed, repeating the session in those cases in which the improvement was partial. At 6 and 12 months, there were improvements of 75–80% with simple disk herniation, 70% with multiple hernias, and 55% with relapses.
Equally positive results are obtained by Castro et al. (2009), in a prospective observational study in which they treated 41 patients with simultaneous intradiscal, epidural, and periradicular infiltrations. Patients with a herniated disk and free fragment and/or major neurological deficit were excluded. The evolution was very positive (according to the VAS and the Laitinen test) from the first to the last of the post-basal records (at 30 days and 6 months, respectively), and the degree of satisfaction was rated as good by 85.4% of the sample.
To clarify the long term results of this technique, Torres et al. (2009) designed a study in patients with sciatica due to herniated disc by applying three consecutive sessions of O2/O3 infiltrations once a week; the first two with an epidural [adding bupivacaine (5 ml to 0.25%) and triamcinolone (4 mg)] and paravertebral ozone and the third one, only with intradiscal ozone. The evolution of 91 patients was recorded for 24 months. A very significant improvement was achieved in 95.6% of the patients at the first-month follow-up visit, 87.7% at the first-year visit, and persisted at the end of the follow-up in 84.1% of the sample. They got one case of discitis and 11 cases of temporary headache and four cases of temporary low back pain. They found a significant reduction of the size of the hernia in 79% of the patients at 24 months MRI.
Although most of the works published refer to intradiscal injections, paravertebral injections are safer, more simple, and the most used in clinical practice, although their efficacy was under discussion. In 2006, a randomized clinical trial was published (Zambello et al., 2006) comparing the efficacy of muscular paravertebral infiltration of O2/O3 with that of epidural steroids in patients refractory to conventional treatment (oral steroids and muscle relaxants). One hundred and seventy one patients were treated with epidural steroids and 180 underwent paravertebral infiltrations of medical ozone. At the 3 weeks follow-up, the improvement was statistically significant in favor of patients treated with ozone therapy (total or almost total remission of pain in 88.2%, compared to 59% in the steroids group), and at 6 months the evolution was excellent or good in 77.1% of patients treated with ozone therapy, compared to 47.3% of patients treated with steroids.
A double-blind randomized clinical trial was conducted (Paoloni et al., 2009) to better assess the efficacy of paravertebral ozone infiltrations in the treatment of acute low back pain due to herniated disk. Sixty patients were recruited and randomized into two groups; one was treated with real infiltrations and in the other group these were simulated. Follow-up was done 15, 30, 90, and 180 days after ending the treatment. Patients treated with true ozone injections significantly improved the pain and functional limitation (p < 0.05), requiring less analgesic medication.
In 2010, a meta-analysis was published (Steppan et al., 2010) on the efficacy and safety of ozone therapy for the treatment of herniated disks. Twelve studies were included with a total sample of 8,000 patients; the mean improvements recorded were similar to those reported for discectomy: 3.9 points out of 10 on the visual analog pain scale, 25.7 points in functional capacity according to the Oswestry Disability Index and a 79.7% improvement in the records of the modified MacNab scale. The percentage of complications was 0.064%, so the treatment was considered safe and effective. Two years later, Magalhaes et al. (2012) published a systematic review and meta-analysis compiling eight observational studies and four randomized clinical trials. They concluded that the intradiscal injection to treat lumbar disk herniation has a recommendation level of 1C and that the paravertebral treatment has a recommendation level 1B according to the criteria of the US Preventive Services Task Force; this means that the recommendation is strong (maximum level), although with certain reservations for intradiscal injection due to the diversity of existing protocols.
About 80% of the population in Western countries will experience at least one episode of low back pain in your lifetime, and 55% of these will have an associated radicular pain (Long, 1991). Failed back surgery syndrome ranges between 15% and 20%, which leads to propose more conservative and less invasive treatments, such as ozone therapy, whose effectiveness seems to oscillate between 65 and 80% suggesting that a small change in disk volume can produce a large clinical change (Gangi et al., 1998). Complications of open surgery must also be taken into account, such as fibrosis, epidural and perineural tears, nerve adhesions, limitations of biomechanics due to fibrosis, and muscle paravertebral spasms and associated myofascial syndromes (Manchikanti et al., 2007). In this context, infiltrations with O2/O3, both at the paravertebral level and trigger points of related musculature and percutaneous intradiscal injection with ozone, are techniques on the rise due to their efficacy, ease of execution, low cost, and very few important side effects.
Andreula et al. (2003), when comparing ozone intradiscal injection with enzymatic nucleolysis, conclude that, with similar clinical results, treatment with ozone therapy would be the first choice due to its advantages like the ones that follow:
•There is no possibility of allergic reactions or anaphylactic
•Possibility of repeating the treatment as many times as it is considered
•Theoretical lower risk of infections, due to the germicides properties of ozone
•Possibility of using a thinner needle due to ozone fluidity and, therefore, a so much less traumatic injection
•Less post-infiltration discomfort (2, 3 days vs. 1 or 2 weeks).
To these advantages would be added those described over corticosteroids due to the absence of ozone adverse effects. In this regard, Fernández et al. (1998), in their review on the use of corticosteroids draw attention to the following points:
•Infectious arthritis
•Progressive joint deterioration
•Soft-tissue atrophy and hypopigmentation
•Tendon rupture
•Reactive synovitis due to glucocorticoid microcrystals
•Systemic adverse effects.
Some recent publications remark that the ozone administration does not close the path to surgery in case of failure (Bocci et al., 2015; Muto et al., 2016).
Finally, it is worth mentioning that the efficacy of ozone therapy in the treatment of failed back surgery syndrome, highly prevalent among spine-operated patients, and usually worsens with new surgeries. In these patients, we observe fibrosis due to epidural and perineural scars, paravertebral spasms, and neural adhesions, whose chronic inflammatory stimulus would lead to neuroplastic phenomena with central and peripheral sensitization. Theoretically, the fibrinolytic, anti-inflammatory and antioxidant properties of the infiltrated O2/O3 would make it ideal for the treatment of these processes. The team from the National Medical Center 20 de Noviembre, in Mexico City, has published two papers treating 30 patients in each work. On both studies applied a first epidural injection together paravertebral infiltration followed by three weekly sessions of paravertebral infiltrations; doses of 20 ml at 30 μg/ml in the first paper and the same amount at 50 μg/ml in the second one, but the treatments could not improve patients’ pain (Grijalva et al., 2012; Hernández et al., 2012). A promising alternative would be the combination of repeated paravertebral injections combined with epidural ones. Padilla del Rey et al. (2015) reported very significant improvement (VAS of 10 a 3) in a patient with refractory post-laminectomy pain who received three epidural infiltrations with ozone (10 ml at 20 μg/ml concentration) in three consecutive weeks and six paravertebral infiltrations, twice a week at the same time (10 ml at 10–30 μg/ml progressive concentration). Anyway, given the scale of the problem, more studies are needed.
Infiltrative Ozone Therapy in Rheumatoid Arthritis
A preclinical study carried out in Nanfang Hospital compared the effects of medical ozone infiltrations at different concentrations compared to oxygen; the authors showed that intra-articular ozone injected at a concentration of 40 μg/ml is capable of inhibiting synovitis in rats with rheumatoid arthritis (Chen et al., 2013). Some doctors use ozone therapy empirically in patients with rheumatic diseases using joint infiltrations for years, supposedly with very positive results, but there are no major works published in this regard.
As mentioned, ozone therapy would be indicated as an adjuvant treatment of diseases related to disturbance of cellular redox balance or tissue oxygenation. From this point of view, systemic ozone therapy would help patients with pain chronic, as recent preclinical studies have demonstrated the role of ROS in hyperalgesia, via activation of the N-methyl-D-aspartate (NMDA) receptors. Gao et al. (2007), in a preclinical model of pain, both neuropathic and inflammatory, could demonstrate that ROS were increased at the dorsal horn in these patients, and that systemic administration of a neutralizing agent of ROS reduced the hyperalgesia by blocking phosphorylation from NMDAs. Later, the same research group (inducing hyperalgesia by capsaicin in rats) was able to demonstrate the role of the superoxide anion as responsible for abnormal pain signal processing in the dorsal horn, suggesting the therapeutic role of mitochondrial SOD-2 in these types of pain (Schwartz et al., 2009).
But certainly, the levels of scientific evidence in the treatment with systemic ozone therapy for chronic pain are practically non-existent. In this regard, a study by Clavo et al. (2013), on chronic headache refractory to triptans, found that systemic ozone improved pain and frequency of crises. Also, Fernández et al. (2016) published a work in which the use of systemic ozone therapy improved efficacy and decreased the side effects of methotrexate in patients with rheumatoid arthritis. Theoretically, the beneficial effect on immunosuppressed patients would make it useful, both in the treatment of herpes zoster infection and postherpetic neuralgia (Hu et al., 2018). In this field, several experts have tried ozone treatments for years, apparently with positive results. Ozone therapy is generally used as an adjunct to conventional treatments, either systemic or local (infiltrations or applications of oils and ozonated water; Mattassi et al., 1985; Delgado et al., 1989; Konrad, 2001). These studies have a low evidence level but are useful to encourage the development of better-designed works.
Fibromyalgia seems to be a “stress disease” in which underlies an alteration of the cellular redox balance, consequence of an increase in the production of free radicals, a deficiency of organic antioxidant capacity, or both simultaneously. Biochemical findings support this fact and systemic ozone therapy has been proposed (Borrelli and Bocci, 2002; Hidalgo, 2012). Hidalgo et al. (2005) treated 21 patients with fibromyalgia refractory to a multidisciplinary treatment with 10 sessions of autohemotherapy, finding very good tolerability and improvement in pain and fatigue, as well as a significant decrease in the use of pain medication. This same research group (Hidalgo-Tallón et al., 2013) treated 36 patients with fibromyalgia with one daily dose of rectal ozone (200 ml of gas at 40 μg/ml) during 24 sessions, reporting significant improvements in the Fibromyalgia Impact Questionnaire, the state of mind, and the physical component of the quality of life using SF-12 scale. The treatment was very well tolerated, with transient meteorism as the most relevant adverse effect.
Systemic ozone has also been tested together with infiltrations in patients with rheumatoid arthritis. A Calunga et al. (2007) research group, published a study about lumbar disk herniation comparing paravertebral infiltrations isolated or combined with rectal ozone and checked that the combination improved all clinical parameters. In 2010, they compared (Méndez-Pérez et al., 2010) isolated O2/O3 intra-articular infiltrations (3 ml at 10 μg/ml) with the infiltrations plus rectal ozone in patients with rheumatoid arthritis of the temporomandibular joint; improvements, both in pain and in function and state of the joint capsule were statistically significant in favor of the combination therapy. In this regard, systemic ozone therapy seems to decrease in these patients interleukin 1 beta levels, directly related to disease activity, while intraarticular ozone injections would decrease intraarticular interleukin 8 levels, justifying lower granulocyte count and clinical improvement (Eastgate et al., 1988; Menéndez et al., 1989; Fahmy, 1993, 1995).
Safety and Contraindications of Ozone Therapy
All authors agree on the high safety of treatments with ozone therapy, especially modern medical ozone generators with great precision.
Jacobs (1982) published that the incidence of effects adverse effects of systemic ozone therapy was only 0.0007%, mainly nausea, headache, and fatigue. In Cuba, with 25 years of experience, having at least one ozone therapy unit per province of the country, only slight adverse effects have been recorded (Bocci, 2002).
The experience of Italian experts is similar, although Dr. Bocci (Ajamieh et al., 2005) describes at least six deaths from gas applications in a direct intravenous way, a practice not recommended by scientific associations (Baeza et al., 2015).
Eventually, the most serious common adverse effect would be a vagal reaction, generally associated with pain during infiltration. It is necessary to note that the injection must be done slowly, especially if a large gas volume at a high concentration is used (Zambello et al., 2004).
An absolute contraindication is severe glucose-6 deficiency phosphate dehydrogenase (favism), as this enzyme is necessary for supply hydrogen ions to the glutathione system, responsible for buffering the oxidation that lipoperoxides will produce in red blood cells (Viebahn, 2007).
As relative contraindications to systemic ozone therapy would be uncontrolled hyperthyroidism, thrombocytopenia, severe cardiovascular instability, and seizure states. It is also not advisable to use systemic ozone therapy in pregnant patients (Bocci, 2002) as it has not been deeply tested. Infiltrations should be avoided following the general criteria described in the literature (Sánchez et al., 2006).
Undoubtedly, ozone therapy should be practiced by a well-trained doctor and, in patients with a poor general condition, a diagnosis of the pro-oxidant/antioxidant status of the patient would be advisable.
Conclusion
For knee osteoarthritis and lumbar disk herniation, evidence on safety and efficacy from systematic reviews and meta-analysis, according the quality of the evidences proposed by the Scottish Intercollegiate Guidelines Network (SIGN), including GRADE criteria, are high (1+ and 2+ studies) and allow a recommendation level B, the same observed in most of the techniques used presently in pain units (SIGN, 2019).
However, for the rest of potential indications, the evidence level is low and ozone must be used only when other conventional treatments have failed or in a compassionate way.
Lack of standardization in treatment protocols is the Achilles’ heel of this technique, probably because of his great tolerablity that encourage doctors to explore different dosages without comparing efficacy between them. This is the main criticism in systematic reviews’ conclusions.
More RCT are needed to increase our knowledge on the indications of medical ozone, but safety profile is good enough so as to develop them. Fortunately, research interest on ozone therapy is growing, as we can check by simply doing a basic research in PubMed and watching the evolution of the number of publications in the past 20 years.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Ajamieh, H. H., Berlanga, J., Merino, N., Sánchez, G. M., Carmona, A. M., Cepero, S. M., et al. (2005). Role of protein synthesis in the protection conferred by ozone – oxidative – preconditioning in hepatic ischemia/reperfusion. Transpl. Int. 18, 604–612. doi: 10.1111/j.1432-2277.2005.00101.x
Ajamieh, H. H., Menéndez, S., Martínez-Sánchez, G., Candelario-Jalil, E., Re, L., Giuliani, A., et al. (2004). Effects of ozone oxidative preconditioning on nitric oxide generation and cellular redox balance in a rat model of hepatic ischemia – reperfusion. Liver Int. 24, 55–62. doi: 10.1111/j.1478-3231.2004.00885.x
Ajamieh, H. H., Menéndez, S., Merino, N., Martinez-Sanchez, G., Re, L., and León, O. S. (2003). Ischemic and ozone oxidative preconditioning in the protection against hepatic ischemic-reperfusion injury. Ozone Sci. Eng. 25, 241–250. doi: 10.1080/01919510390481568
Alexandre, A., Coro, L., Azuelos, A., Buric, J., Salgado, H., Murga, M., et al. (2005). “Intradiscal injection of oxygen-ozone gas mixture for the treatment of cervical disc herniations,” in Advanced Peripheral Nerve Surgery and Minimal Invasive Spinal Surgery. ed. A. Alexandre. Vienna: Springer.
Andreula, C. F., Simonetti, L., De Santis, F., Agati, R., Ricci, R., and Leonardi, M. (2003). Minimally invasive oxygen-ozone therapy for lumbar disk herniation. Am. J. Neuroradiol. 24, 996–1000.
Anzolin, A. P., and Bertol, C. D. (2018). Ozonioterapia como terapêutica integrativa no tratamento da osteoartrose: uma revisão sistemática. Br. J. Pain 1, 171–175. doi: 10.5935/2595-0118.20180033
Arias-Vázquez, P. I., Tovilla-Zárate, C. A., Bermudez-Ocaña, D. Y., Legorreta-Ramírez, B. G., and López-Narváez, M. L. (2019). Eficacia de las infiltraciones con ozono en el tratamiento de la osteoartritis de rodilla vs. otros tratamientos intervencionistas: revisión sistemática de ensayos clínicos. Rehabilitación. 53, 43–55. doi: 10.1016/j.rh.2018.11.001
Babaei-Ghazani, A., Karimi, N., Forogh, B., Madani, S. P., Ebadi, S., Fadavi, H. R., et al. (2019). Comparison of ultrasound-guided local ozone (O2-O3) injection vs corticosteroid injection in the treatment of chronic plantar fasciitis: a randomized clinical trial. Pain Med. 20, 314–322. doi: 10.1093/pm/pny066
Balan, C., Schiopu, M., Balasa, D., and Balan, C. (2017). Ozone therapy – a rare and avoidable source of infectious pathology of the spine. Rom Neurosurg. 31:46. doi: 10.1515/romneu-2017-0046
Balkanyi, A. (1989). “The interaction between ozone therapy and oxygen radicals and their importance in practice.” in Proceedings of the Ninth Ozone World Congress; June 3–9, 1989; New York; 22–27.
Barber, E., Menéndez, S., Barber, M. O., Merino, N., and Calunga, J. L. (1998). Functional and morphological renal study in kidneys of rats pretreated with ozone and subjected to warm ischemia. CENIC Biol. Sci. 29, 178–181.
Bocci, V., Borrelli, E., Zanardi, I., and Travagli, V. (2015). The usefulness of ozone treatment in spinal pain. Drug Des. Devel. Ther. 9:2677. doi: 10.2147/DDDT.S74518
Bonetti, M. (2003). CT-guided oxygen-ozone infiltration into isthmic lysis points in the management of 1st negree spondylolisthesis and spondylolysis. Riv. Ital. Ossigeno-Ozone Ther. 2, 31–38.
Bonetti, M., Cotticelli, B., Richelmi, P., and Valdenassi, L. (2002). Rofecoxib e O2-O3 therapy vs O2-O3 therapy in the spondyloarthrosis treatment. Riv. Ital. Ossigeno-Ozone Ther. 1, 171–178.
Bonetti, M., Fontana, A., Cotticelli, B., Dalla Volta, G., Guindani, M., and Leonardi, M. (2005). Intraforaminal O2-O3 versus periradicular steroidal infiltrations in lower back pain: randomized controlled study. Am. J. Neuroradiol. 26, 996–1000.
Bonetti, M., Moretti, M., Guarino, G., and Bragaglio, G. (2011). Rhizoarthrosis: our experience with oxygen-ozone treatment. Riv. Ital. Ossigeno-Ozone Ther 10, 63–63.
Borrelli, E., and Bocci, V. (2002). A novel therapeutic option for chronic fatigue syndrome and fibromyalgia. Riv. Ital. Ossigeno-Ozone Ther. 1, 149–153.
Brina, L., and Villani, P. C. (2004). Treatment of rotator cuff lesions with echo-guided infiltration of an oxygen-ozone mixture. Riv. Ital. Ossigeno-Ozone Ther. 3, 139–147.
Buric, J. (2005). Ozone chemyonucleolysis vs microdiscectoy. Prospective controlled study with 18 months follow-up. Riv. Ital. Ossigeno-Ozone Ther. 4, 49–54.
Calunga, J. L., Ramos, T. L., Castillo, P., Menéndez, S., Carballo, A., and Céspedes, J. (2007). Ozonoterapia combinada en el tratamiento del paciente portador de hernia discal lumbar: estudio preliminar. Rev Cubana Invest Bioméd [Internet]. 2007 Mar [cited 2021 Nov 30]; 26. Available in: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-03002007000100003&lng=esn
Cano, P. A., Vela, T., Cano, C., García, G., Vera, J. C., and Andrés-García, J. A. (2016). Cervical spondylodiscitis after oxygen–ozone therapy for treatment of a cervical disc herniation: a case report and review of the literature. HSSJ. 12, 278–283. doi: 10.1007/s11420-016-9500-1
Chen, H., Yu, B., Lu, C., and Lin, Q. (2013). The effect of intra-articular injection of different concentrations of ozone on the level of TNF-α, TNF-R1, and TNF-R2 in rats with rheumatoid arthritis. Rheumatol. Int. 33, 1223–1227. doi: 10.1007/s00296-012-2529-7
Corea, F., Amici, S., Murgia, N., and Tambasco, N. (2004). A case of vertebrobasilar stroke during oxygen-ozone therapy. J. Stroke Cerebrovasc. Dis. 13, 259–261. doi: 10.1016/j.jstrokecerebrovasdis.2004.08.004
Escarpanter, J. C., Valdés, O., Sánchez, R., López, Y., and López, C. (1997). Therapeutic results in osteoarthritis of the knee with ozone infiltrations. Rev. Cuba. Investig. Biomed. 16, 124–132.
Fahmy, Z. (1993). “Immunological effect of ozone (O2-O3) in rheumatic diseases.” in Proceedings of the Eleventh Ozone World Congress, Ozone in Medicine. (Stamford, Conn.: International Ozone Association); August 29 - September 3, 1993; San Francisco, CA, USA.
Fahmy, Z. (1995). “Correlation of plasma interleukin 1 levels with disease activity in rheumatoid arthritis with and without Ozone.” in Proceedings of the 12th Ozone World Congress (Stamford, Conn.: International Ozone Association); May 15-18, 1995; Lille, France.
Fernández, O. S. L., Viebahn-Haensler, R., Cabreja, G. L., Espinosa, I. S., Matos, Y. H., Roche, L. D., et al. (2016). Medical ozone increases methotrexate clinical response and improves cellular redox balance in patients with rheumatoid arthritis. Eur. J. Pharmacol. 789, 313–318. doi: 10.1016/j.ejphar.2016.07.031
Fernández-Cuadros, M. E., Pérez-Moro, O., Albaladejo-Florin, M. J., and Álava-Rabasa, S. (2020). El ozono intrarticular modula la inflamación, mejora el dolor, la rigidez, la función y tiene un efecto anabólico sobre la artrosis de rodilla: estudio cuasiexperimental prospectivo tipo antes-después, 115 pacientes. Rev Soc Esp Dolor. 27, 78–88. doi: 10.20986/resed.2020.3775/2019
Fort, N. M., Aichmair, A., Miller, A. O., and Girardi, P. (2014). L5–S1 Achromobacter xylosoxidans infection. Spine 39, E413–E416. doi: 10.1097/BRS.0000000000000195
Fuccio, C., Luongo, C., Capodanno, P., Giordano, C., Scafuro, M. A., Siniscalco, D., et al. (2009). A single subcutaneous injection of ozone prevents allodynia and decreases the over-expression of pro-inflammatory caspases in the orbito-frontal cortex of neuropathic mice. Eur. J. Pharmacol. 603, 42–49. doi: 10.1016/j.ejphar.2008.11.060
Gaffuri, M., Garaffo, R., and Gheza, G. (2003). Oxygen-ozone therapy for lateral humeral epicondylitis: preliminary findings. Riv. It Ossigeno-Ozone Ther. 2, 169–172.
Gangi, A., Dietemann, J. L., Mortazavi, R., Pfleger, D., Kauff, C., and Roy, C. (1998). CT-guided interventional procedures for pain management in the lumbosacral spine. Radiographics 18, 621–633. doi: 10.1148/radiographics.18.3.9599387
Gao, X., Kim, H. K., Chung, J. M., and Chung, K. (2007). Reactive oxygen species (ROS) are involved in enhancement of NMDA-receptor phosphorylation in animal models of pain. Pain 131, 262–271. doi: 10.1016/j.pain.2007.01.011
Gazzeri, R., Galarza, M., Neroni, M., Esposito, S., and Alfieri, A. (2007). Fulminating septicemia secondary to oxygen-ozone therapy for lumbar disc herniation. Case Rep. 32, E121–E123. doi: 10.1097/01.brs.0000254125.85406.6e
Gheza, G. (2002). Metatarsalgia trattata with O2-O3 in peace with fibrosis post-chirurgical scarring of Morton’s neuroma asportazione. Riv. Ital. Ossigeno-Ozone Ther. 1, 109–111.
Gheza, G., Ipprio, L., and Bissolotti, L. (2002). Oxygen-ozone therapy in a diabetic patient with De Quervain’s tenosynovitis associated with joint arthrosis. Riv. Ital. Ossigeno-Ozone Ther. 1, 189–192.
Ginanneschi, F., Cervelli, C., Milani, P., and Rossi, A. (2006). Ventral and dorsal root injury after oxygen-ozone therapy for lumbar disk herniation. Surg. Neurol. 66, 619–620. doi: 10.1016/j.surneu.2006.01.025
Giombini, A., Menotti, F., Di Cesare, A., Giovannangeli, F., Rizzo, M., Moffa, S., et al. (2016). Comparison between intrarticular injection of hyaluronic acid, oxygen ozone, and the combination of both in the treatment of knee osteoarthrosis. J. Biol. Regul. Homeost. Agents 30, 621–625.
Gjonovich, A., Girotto, L., Sattin, G. F., Girotto, T., and Preciso, G. (2002). Oxygen-ozone therapy in shoulder pain. Riv. Ital. Ossigeno-Ozone Ther. 1, 37–40.
Gjonovich, A., Marchetto, R., Montemarà, E., and Girotto, T. (2003). Refractory tendinopathies of the knee: use of oxygen-ozone therapy. Riv. Ital. Ossigeno-Ozone Ther. 2, 187–192.
Grijalva, Y. M., Hernández, J. R., Tenopala, S., Canseco, C. P., and Torres, J. C. (2012). Application efficiency of epidural and paravertebral ozone at a concentration of 50 μg/ml in patients with chronic pain secondary to postlaminectomy syndrome. Rev. Soc. Esp Dolor. 19, 66–71.
Gurger, M., Once, G., Yilmaz, E., Demir, S., Calik, I., Say, Y., et al. (2021). The effect of the platelet-rich plasma and ozone therapy on tendon-to-bone healing in the rabbit rotator cuff repair model. J. Orthop. Surg. Res. 16:202. doi: 10.1186/s13018-021-02320-w
Hawkins, C. L., and Davies, M. J. (1996). Direct detection and identification of radicals generated during the hydroxyl radical-induced degradation of hyaluronic acid and related materials. Free Radic. Biol. Med. 21, 275–290. doi: 10.1016/0891-5849(96)00042-1
He, R., Huang, Q., Yan, X., Liu, Y., Yang, J., and Chen, X. (2019). A case of paradoxical embolism causing anterior spinal cord syndrome and acute myocardial infarction following the Intradiscal oxygen-ozone therapy. Front. Neurol. 10:137. doi: 10.3389/fneur.2019.00137
Hernández, B. D., Hernández, J. R., Tenopala, S., Canseco, C. P., and Torres, J. C. (2012). Application efficiency epidural and paravertebral ozone at a concentration of 30 μg/ml for the management of chronic pain in patients with failed surgery syndrome back. Rev. Soc. Esp Dolor. 19, 3–10.
Hidalgo, F. J., Calandre, E., Rico, F., Delgado, A., Entrena, J. M., and Menéndez, S.. (2005). “Interest of systemic ozone in the treatment of highly refractory fibromyalgia.” in IV Jornadas Nacionales de Oxígeno-ozonoterapia médica. Noviembre 4-5, 2005; Sevilla (Spain).
Hidalgo-Tallón, F. J., Menéndez-Cepero, S., Vilchez, J. S., Rodríguez-López, C. M., and Calandre, E. P. (2013). Ozone therapy as add-on treatment in fibromyalgia management by rectal insufflation: an open-label pilot study. J. Altern. Complement. Med. 19, 238–242. doi: 10.1089/acm.2011.0739
Hu, B., Zheng, J., Liu, Q., Yang, Y., and Zhang, Y. (2018). The effect and safety of ozone autohemotherapy combined with pharmacological therapy in postherpetic neuralgia. J. Pain Res. 11, 1637–1643. doi: 10.2147/JPR.S154154
Huanqui, C., Cruz, M., Miranda, A., Poblete, P., and Mamani, R. (2006). Effectiveness and safety of intra-articular ozone in knee osteoarthritis refractory to treatment. UCSM 12, 21–26.
Hüseyin, T., Uğur, Ö., Hasan, K., and Nurettin, L. (2017). Severe headache following ozone therapy: Pneumocephalus. Agri 29, 132–136. doi: 10.5505/agri.2016.36024
Ikonomides, S. T., Iliakis, E. M., Eleftheriadou, A., Bratanis, D., and Thomaidis, R. (2003). Conservative treatment of acute or chronic tendonitis with oxygen-ozone mixture. Riv. Ital. Ossigeno-Ozone Ther. 2, 67–71.
Ikonomidis, S. T., Iliakis, E. M., and Charalambus, L. (2002). Nonoperative treatment of shoulder impingement syndrome with topical injections of medical oxygen-ozone mixture. A double blind clinical trial. Riv. Ital. Ossigeno-Ozone Ther. 1, 41–44.
Iliakis, E., Valadakis, V., Vynios, D. H., Tsiganos, C. P., and Agapitos, E. (2001). Rationalization of the activity of medical ozone on intervertebral disc a histological and biochemical study. Riv. Neuroradiol. 14, 23–30. doi: 10.1177/19714009010140S105
Konrad, H. (2001). “Ozone therapy for postherpetic neuralgia. A retrospective study of 55 cases.” in Proceedings of the 15th Ozone World congress, Medical Therapy Conference (Stamford, Conn.: International Ozone Association). September 11-15, 2011; London, UK.
Leonardi, M., Simonetti, L., and Barbara, C. (2001). Effetti dell’ozono sul nucleo polposo: reperti anatomo-pathologici its an operative case. Riv. Neuroradiol. 14, 57–59. doi: 10.1177/19714009010140S113
Li, Q., Qi, X., and Zhang, Z. (2018). Intra-articular oxygen-ozone versus hyaluronic acid in knee osteoarthritis: A meta-analysis of randomized controlled trials. Int. J. Surg. 58, 3–10. doi: 10.1016/j.ijsu.2018.08.007
Lo Giudice, G., Valdi, F., Maurizio, G., Prosdocimo, G., and de Belvis, V. (2004). Acute bilateral vitreo-retinal hemorrhages following oxygen-ozone therapy for lumbar disk herniation. Am. J. Ophth. 138, 175–177. doi: 10.1016/j.ajo.2004.02.059
Lopes de Jesus, C. C., Dos Santos, F. C., de Jesus, L. M. O. B., Monteiro, I., Sant’Ana, M. S. S. C., and Trevisani, V. F. M. (2017). Comparison between intra-articular ozone and placebo in the treatment of knee osteoarthritis: a randomized, double-blinded, placebo-controlled study. PLoS One 12:e0179185. doi: 10.1371/journal.pone.0179185
Magalhaes, F. N., Dotta, L., Sasse, A., Teixeira, M. J., and Fonoff, E. T. (2012). Ozone therapy as a treatment for low back pain secondary to herniated disc: a systematic review and meta-analysis of randomized controlled trials. Pain Physician 15, E115–E129.
Manchikanti, L., Singh, V., Cash, K. A., Pampati, V., and Datta, S. (2007). Preliminary results of a randomized, equivalence trial of fluoroscopic caudal epidural injections in managing chronic low back pain: part 3 – post surgery syndrome. Pain Physician 11, 817–831.
Marchetti, D., and La Monaca, G. (2000). An unexpected death during oxygen-ozone therapy. Am. J. Forensic Med. Pathol. 21, 144–147. doi: 10.1097/00000433-200006000-00010
Mattassi, R., Bassi, P., D’Angelo, F., Franchina, A., and Sbrascini, S. (1985). “Ozone as therapy in herpes simplex and herpes zoster diseases,” in Medical Applications of Ozone. ed. J. LaRous (Norwalk: International Ozone Association), 134–137.
Méndez-Pérez, I., Cerro-Montesino, A. D., Cámbara-Peña, R., Martínez-Godíne, J., and Menéndez-Cepero, S. (2010). Systemic and intra-ozone therapy joint in arthritis of the temporomandibular joint from arthritis rheumatoid. CENIC Biol. Sci. 41, 169–172.
Menéndez, P., García, A., and Peláez, R. (2014). Absceso paravertebral e intraabdominal secundario a ozonoterapia por lumbalgia. Rev. Esp. Cir. Ortop. Traumatol. 58, 125–127. doi: 10.1016/j.recot.2013.06.003
Menéndez, S. A., González, R., Ledea, O. E., Hernández, F. A., León, O. S., and Díaz, M. F. (2008). Ozone Basic Aspects and Clinical Applications. Havana: CENIC.
Moretti, M. (2011). Effect of treatment with O2-O3 and hyaluronic acid in partial tear of the supraspinatus tendon. Riv. Ital. Ossigeno-Ozone Ther. 10:37.
Moretti, B., Lanzisera, R., Morese, A., Moretti, L., Patella, S., Patella, V., et al. (2004a). O2-O3 vs chondroprotectors in the treatment of osteoarthritis of the knee. Riv. Ital. Ossigeno-Ozone Ther. 3, 65–72.
Moretti, B., Lanzisera, R., Pesce, V., Moretti, L., Patella, S., and Patella, V. S. C. (2004b). O2-O3 vs. anti-inflammatory drugs in the treatment of neck pain. Riv. Ital. Ossigeno-Ozone Ther. 3, 131–137.
Mustafa, Ç., Yunus, C., and Şakir, B. (2015). Myocardial infarction after ozone therapy: is ozone therapy Dr. Jekyll or Mr. Hyde? Cardiology 132, 101–104. doi: 10.1159/000431078
Muto, M. (2004). Intradiscal and intramuscular injection of oxygen – ozone: pathological evaluation. Work in Progress. Riv. Ital. Ossigeno-Ozone Ther. 3, 7–13.
Muto, M., Giurazza, F., Silva, R. P., and Guarnieri, G. (2016). Rational approach, technique and selection criteria treating lumbar disk herniations by oxygen–ozone therapy. Interv. Neuroradiol. 22, 736–740. doi: 10.1177/1591019916659266
Noori-Zadeh, A., Bakhtiyari, S., Khooz, R., Haghani, K., and Darabi, S. (2019). Intra-articular ozone therapy efficiently attenuates pain in knee osteoarthritic subjects: a systematic review and meta-analysis. Complement. Ther. Med. 42, 240–247. doi: 10.1016/j.ctim.2018.11.023
Padilla del Rey, M. L., García Fernández, M. R., García Sánchez, F., Rastrollo Peña, D., Díaz-Alejo Marchante, C., and Gonzálvez Ortega, J. J., et al. (2015). “Ozone therapy in failed back surgery syndrome.” in 21st Annual Meeting ESRA. September 30 - October 2, 2015; Mallorca, Spain.
Palanca-Sánchez, I., Puig-Riera de Conías, M. M., Elola-Somoza, J., Bernal-Sobrino, J. L., and Paniagua Caparrós, J. L. (2011). Grupo de Expertos. Unidad de tratamiento de dolor: estándares y recomendaciones. Madrid: Ministerio de Sanidad, Política Social e Igualdad. Available at: https://www.mscbs.gob.es/organizacion/sns/planCalidadSNS/docs/EERR/Unidad_de_tratamiento_del_dolor.pdf (Accessed November 30, 2021).
Paoloni, M., Di Sante, L., Cacchio, A., Apuzzo, D., Marotta, S., Razzano, M., et al. (2009). Intramuscular oxygen-ozone therapy in the treatment of acute back pain with lumbar disc herniation: a multicenter, randomized, double-blind, clinical trial of active and simulated lumbar paravertebral injection. Spine 34, 1337–1344. doi: 10.1097/BRS.0b013e3181a3c18d
Peralta, C., Xaus, C., Bartrons, R., Leon, O. S., Gelpí, E., and Roselló-Catafau, J. (2000). Effect of ozone treatment on reactive oxygen species and adenosine production during hepatic ischemia-reperfusion. Free Radic. Res. 33, 595–605. doi: 10.1080/10715760000301121
Pressman, S. (2021). The story of ozone - 6th edition [Internet]. Santa Barbara Ca: Ozone Therapies Group; 2019 Oct [cited 2021 Nov 30]. Available from: https://www.ozonetherapiesgroup.com/ozone-research/2019/10/28/the-story-of-ozone-6th-edition
Raeissadat, S. A., Tabibian, E., Rayegani, S. M., Rahimi-Dehgolan, S., and Babaei-Ghazani, A. (2018). An investigation into the efficacy of intra-articular ozone (O2-O3) injection in patients with knee osteoarthritis: a systematic review and meta-analysis. J. Pain Res. 11, 2537–2550. doi: 10.2147/JPR.S175441
Salvatore, A., Valente, C., De Benedetti, G., and Caramello, G. (2016). Transient cortical blindness after intradiscal oxygen–ozone therapy. Indian J. Ophthalmol. 64:944. doi: 10.4103/0301-4738.198858
Sánchez, I., Ferrero, A., Aguilar, J. J., Conejero, J. A., Flórez, M. T., Arrebola, A., et al. (2006). SERMEF Manual of Rehabilitation and Physical Medicine. Madrid: Panamerican Medical.
Schwartz, E. S., Kim, H. Y., Wang, J., Lee, I., Klann, E., Chung, J. M., et al. (2009). Persistent pain is dependent on spinal mitochondrial antioxidant levels. J. Neurosci. 29, 159–168. doi: 10.1523/JNEUROSCI.3792-08.2009
Sconza, C., Respizzi, S., Virelli, L., Vandenbulcke, F., Iacono, F., Kon, E., et al. (2020). Oxygen-ozone therapy for the treatment of knee osteoarthritis: a systematic review of randomized controlled trials. Arthroscopy 36, 277–286. doi: 10.1016/j.arthro.2019.05.043
Seyman, D., Sepin, N., Inan, D., Ongu, G., and Ogunc, D. (2012). Pseudomonas aeruginosa septic arthritis of knee after intra-articular ozone injection. New Microbiol. 35, 345–348.
Siemsen, C. H. (1995). Ozon-Anwendung bei akuten und chronischen Gelenkerkrankungen. Ozon-Handbuch. Grundlagen. Prävention. Therapie. Landsberg: Ecomed.
Steppan, J., Meaders, T., Muto, M., and Murphy, K. J. (2010). A metaanalysis of the effectiveness and safety of ozone treatments for herniated lumbar discs. J. Vasc. Interv. Radiol. 21, 534–548. doi: 10.1016/j.jvir.2009.12.393
Torres, L. M., Terrero, M. J., Vidal, M., Aragón, F., and Martínez, J. (2009). Discolysis with intradiscal ozone in the treatment of sciatica due to herniated discs. Follow-up of 100 patients in 24 months. Rev. Soc. Esp. Dolor. 16, 147–152. doi: 10.1016/S1134-8046(09)71006-7
Trenti, G. F., and Gheza, G. (2002). Efficacy of oxygen-ozone pain therapy associated with shock waves to treat calcifying tendinitis of the shoulder. Preliminary findings. Riv. Ital. Ossigeno-Ozone Ther. 1, 45–50.
Vanni, D., Galzio, R., Kazakova, A., Pantalone, A., Sparvieri, A., Salini, V., et al. (2015). Intraforaminal ozone therapy and particular side effects: preliminary results and early warning. Acta Neurochir. 158, 491–496. doi: 10.1007/s00701-015-2545-y
Vilas-Rolan, D., Mila, M., Cuberas, G., Becerra, J. L., Herva, J. V., Massuet, A., et al. (2012). Neurological symptoms following exposure to ozone. J. Neurol. 259, 2740–2742. doi: 10.1007/s00415-012-6667-3
Wang, M. C., Chan, L., Maiman, D. J., Kreuter, W., and Deyo, R. A. (2007). Complications and mortality associated with cervical spine surgery for degenerative disease in the United States. Spine 32, 342–347. doi: 10.1097/01.brs.0000254120.25411.ae
Wen-Juan, T., Long, J., Ying, W., and Ze-Min, K. (2017). Ozone therapy induced sinus arrest in a hypertensive patient with chronic kidney disease: a case report. Medicine 96:e9265.
Xiao, Y. Y., Tian, J. L., Li, J. K., and Zhang, J. S. (2006). CT guided ozone injection for the treatment of cervical disc herniation. Riv. Ital. Ossigeno-Ozone Ther. 5, 109–115.
Yang, C. S., Zhang, L. J., Sun, Z. H., Yang, L., and Shi, F. D. (2018). Acute prevertebral abscess secondary to intradiscal oxygen–ozone chemonucleolysis for treatment of a cervical disc herniation. Int. J. Med. Res. 46, 2461–2465. doi: 10.1177/0300060518764186
Zambello, A., Fara, B., Tabaracci, G., and Bianchi, M. (2006). Epidural steroid injection vs paravertebral O2-O3 infiltration for symptomatic herniated disc refractory to conventional treatment: a prospective randomized study. Riv. Ital. Ossigeno-Ozone Ther. 5, 123–127.
Zanardi, G., and Zorandi, A. (2002). Ossigeno-ozone therapy in the treatment della painful pathology of nell’atleta foot. Riv. Ital. Ossigeno-Ozone Ther. 1, 51–56.
The Venturis Chiropractic and Prolotherapy website uses cookies, tracking pixels and related technologies. By continuing to browse our site, you are agreeing to our use of cookies. OkPrivacy policy


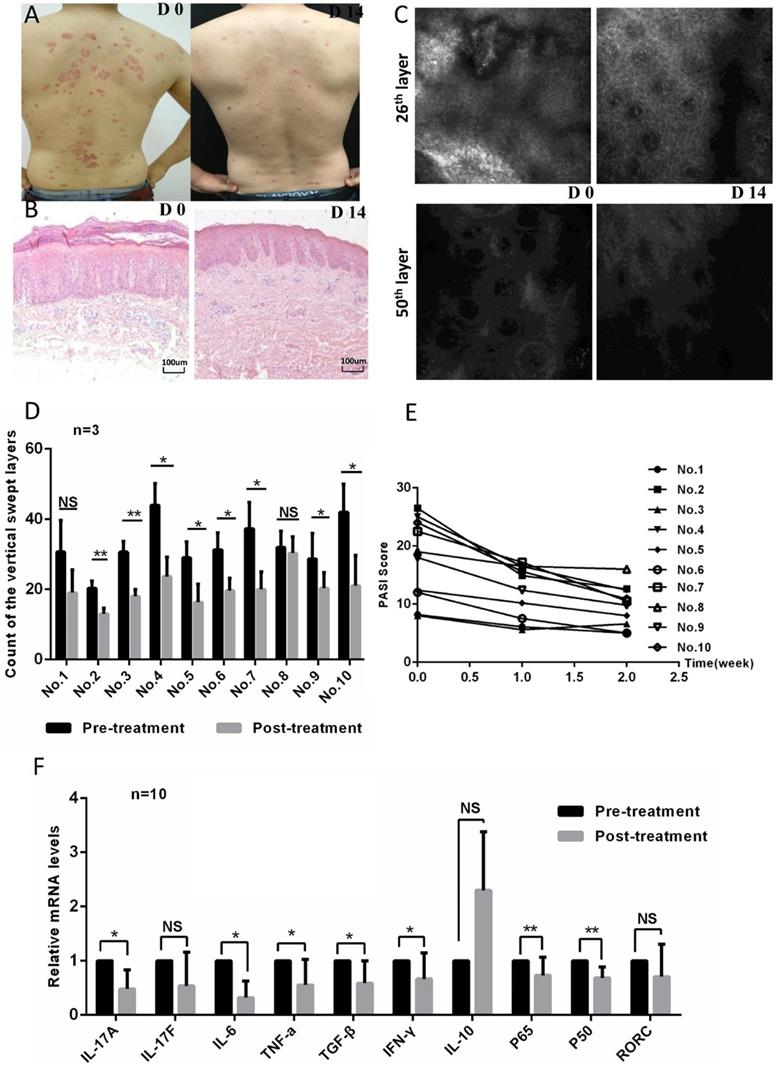
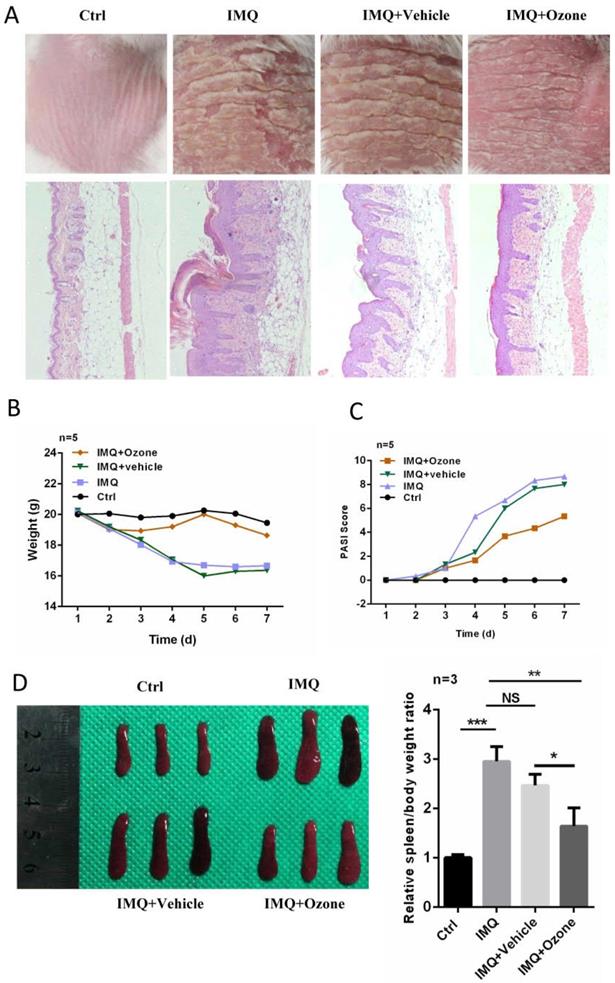
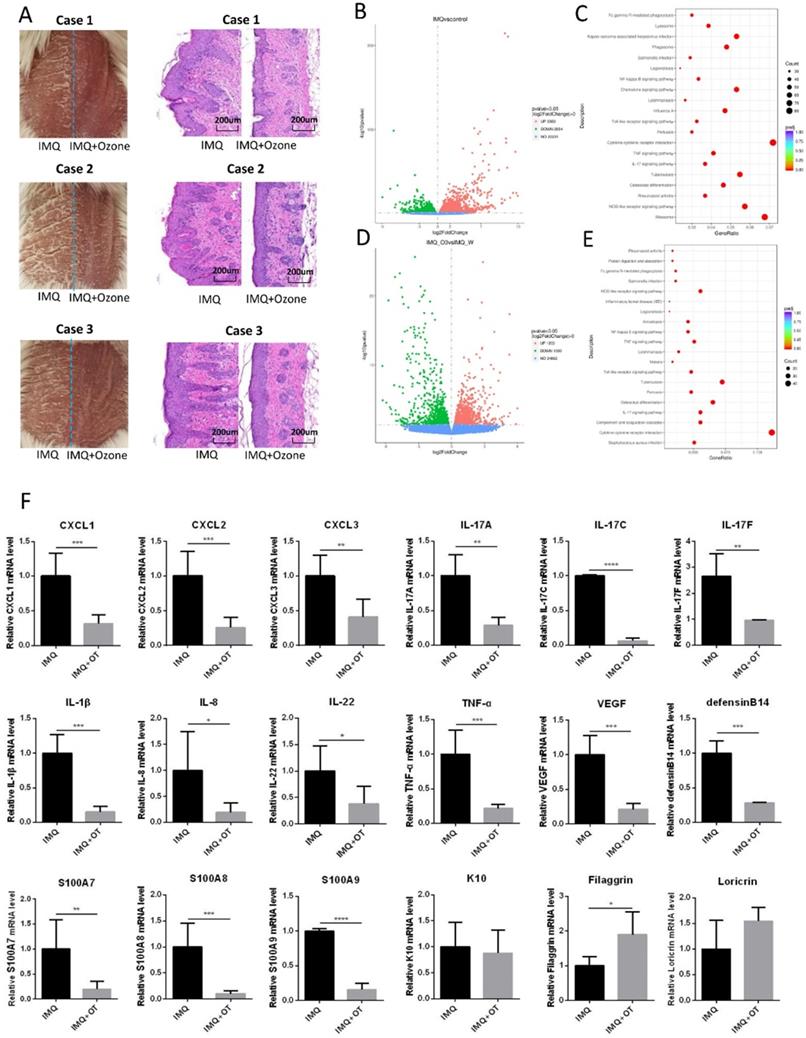
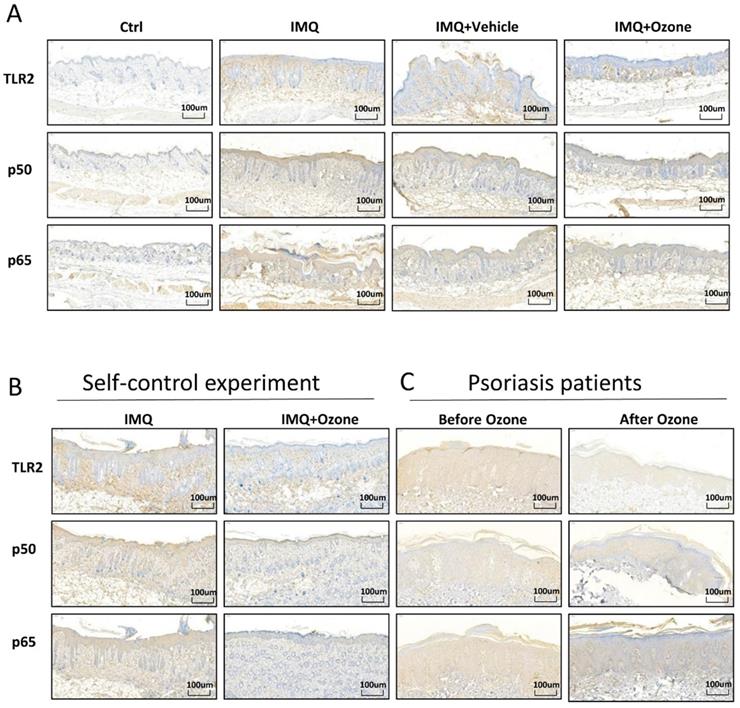
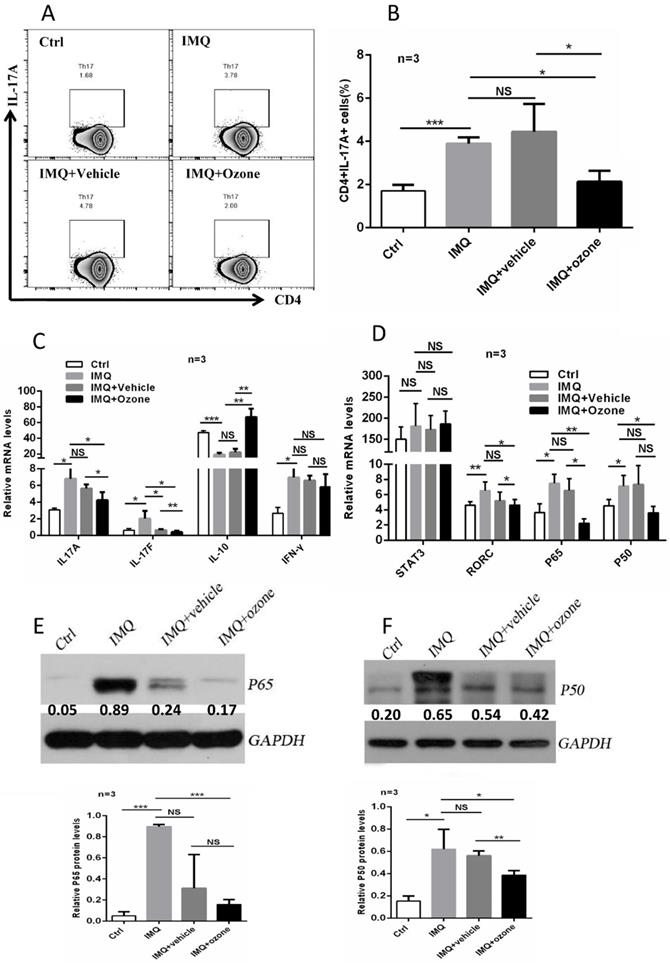
 Francisco Javier Hidalgo-Tallón
Francisco Javier Hidalgo-Tallón Luis Miguel Torres-Morera2
Luis Miguel Torres-Morera2 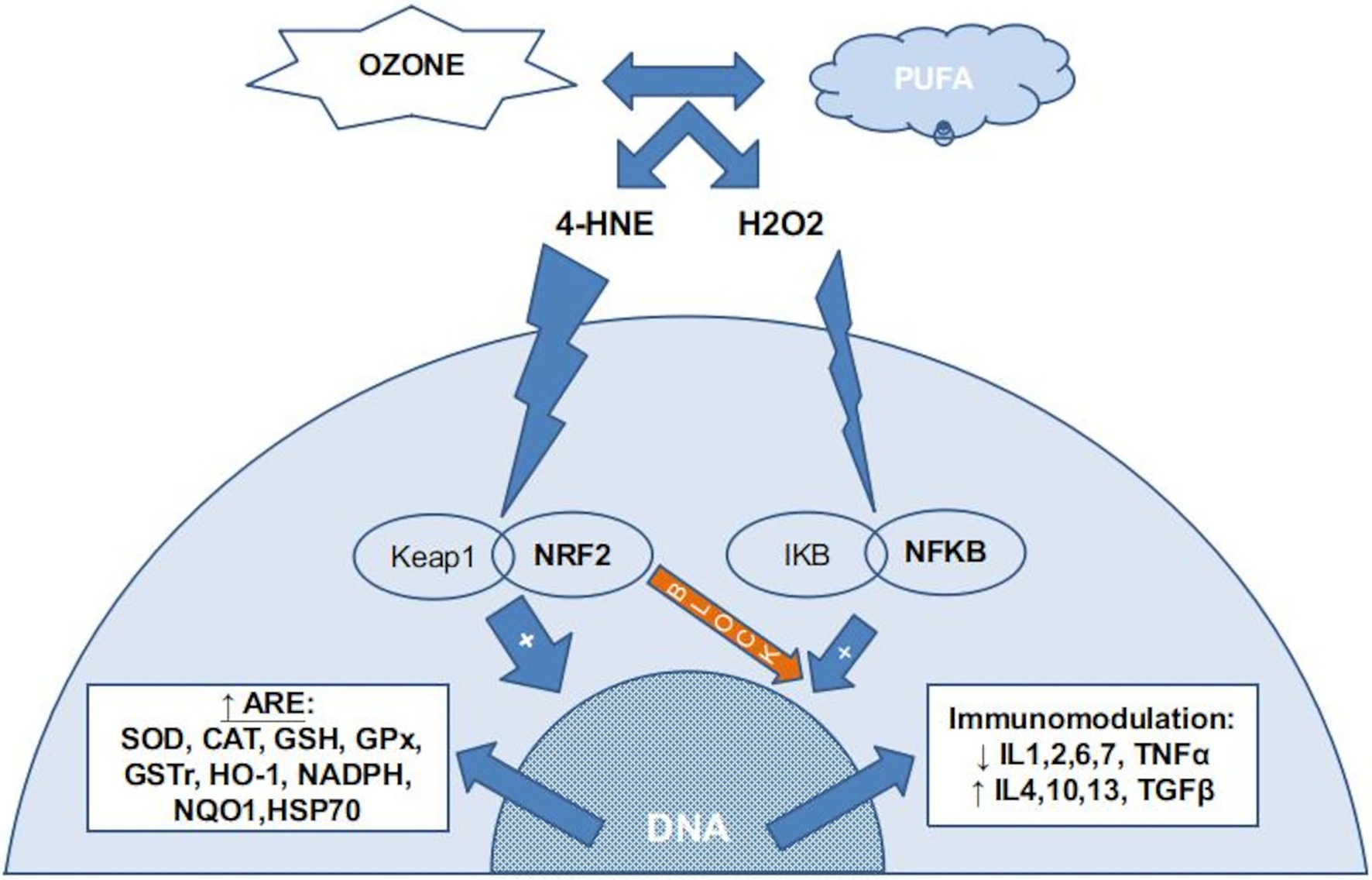 FIGURE 1. The chemical reaction between ozone and PUFA (poli-unsaturated fatty acids) in the insterstitial water (or plasma) produce several ROS, mainly H2O2, and several LOPs, mainly 4-HNE (4-hydroxynonenal). Almost all H2O2 is kidnaped by erythrocytes (not reflected in this figure) if present. In nucleated cells, LOPs activates the NRF2 pathway, inducing the production of ARE (antioxidant response elements) and blocking the NFKB pathway. A small amount of H2O2 stimulates the NFKB pahtway, usually balanced with the NRF2 blocking action, producing a inmmunomodulation.
FIGURE 1. The chemical reaction between ozone and PUFA (poli-unsaturated fatty acids) in the insterstitial water (or plasma) produce several ROS, mainly H2O2, and several LOPs, mainly 4-HNE (4-hydroxynonenal). Almost all H2O2 is kidnaped by erythrocytes (not reflected in this figure) if present. In nucleated cells, LOPs activates the NRF2 pathway, inducing the production of ARE (antioxidant response elements) and blocking the NFKB pathway. A small amount of H2O2 stimulates the NFKB pahtway, usually balanced with the NRF2 blocking action, producing a inmmunomodulation.
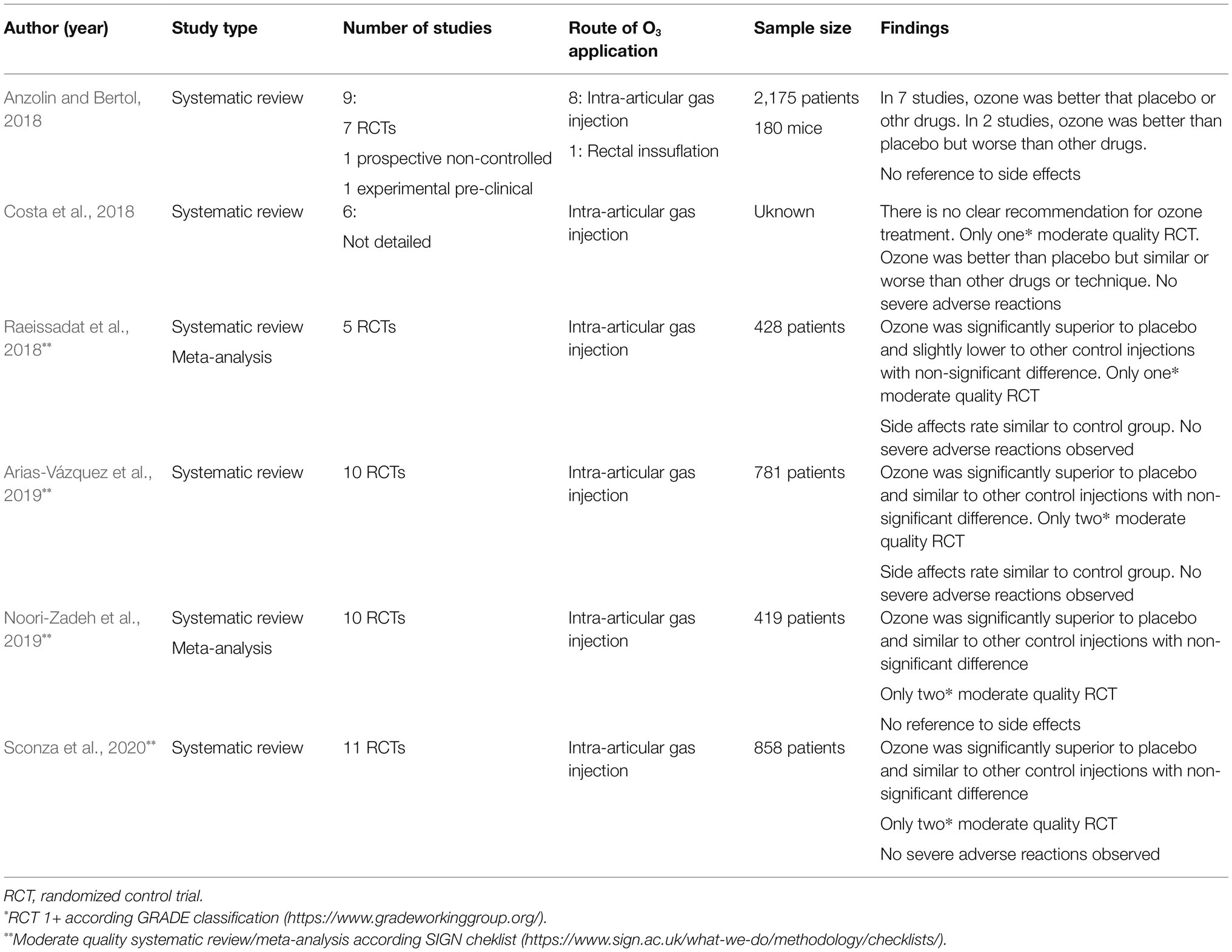 TABLE 1. Systematic reviews and meta-analysis on medical ozone in knee osteoarthritis (Anzolin and Bertol, 2018; Costa et al., 2018; Raeissadat et al., 2018; Arias-Vázquez et al., 2019; Noori-Zadeh et al., 2019; Sconza et al., 2020).
TABLE 1. Systematic reviews and meta-analysis on medical ozone in knee osteoarthritis (Anzolin and Bertol, 2018; Costa et al., 2018; Raeissadat et al., 2018; Arias-Vázquez et al., 2019; Noori-Zadeh et al., 2019; Sconza et al., 2020).

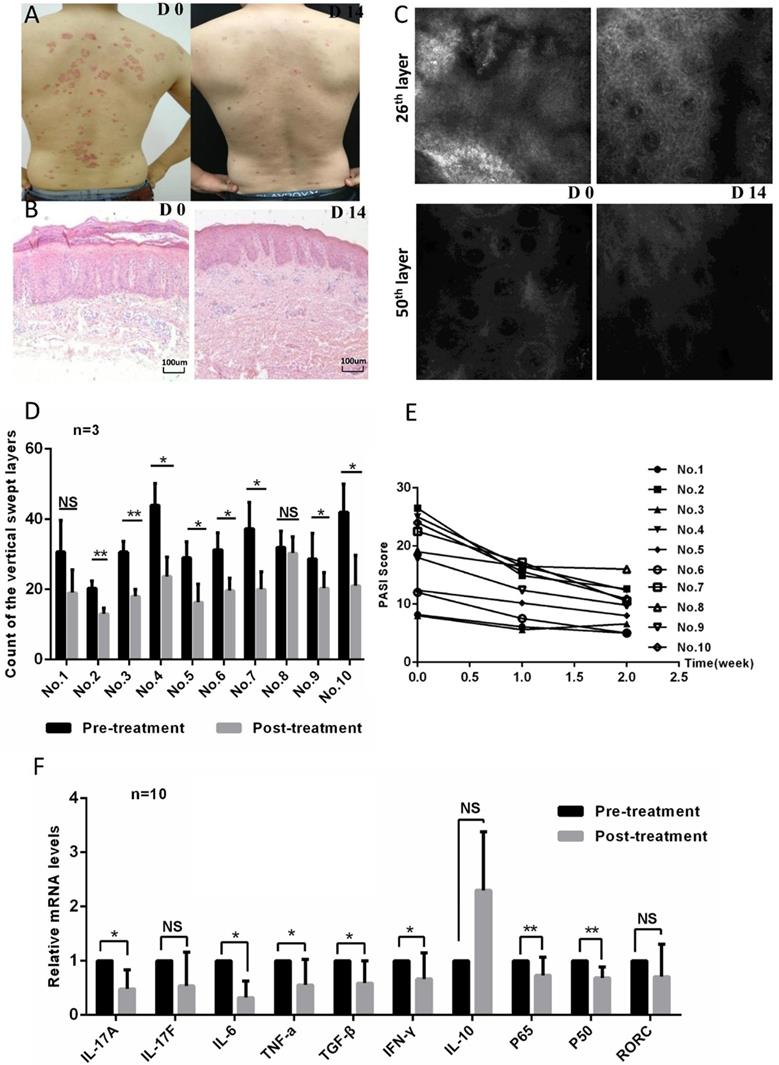{kind=link}
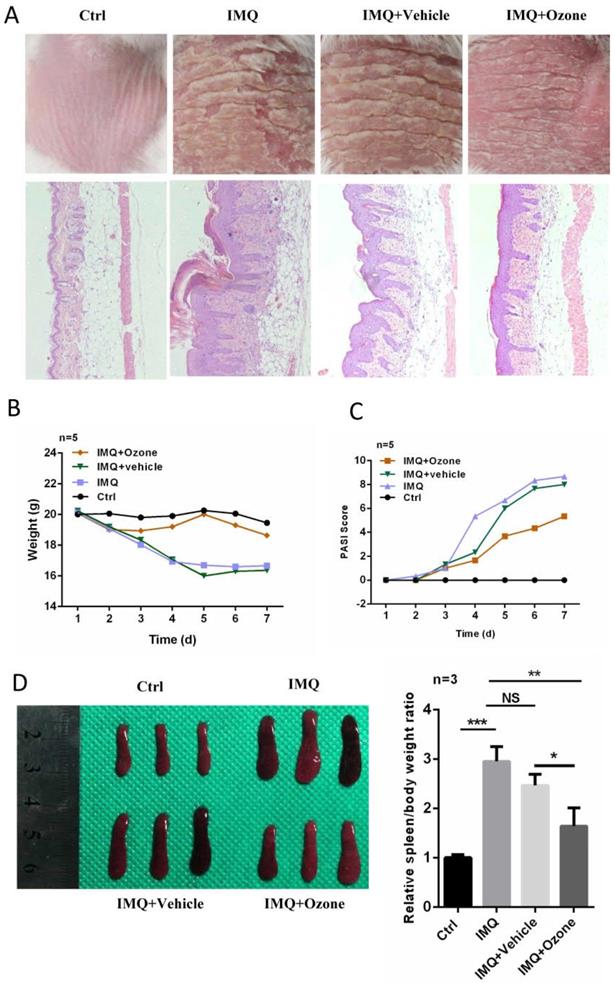{kind=link}
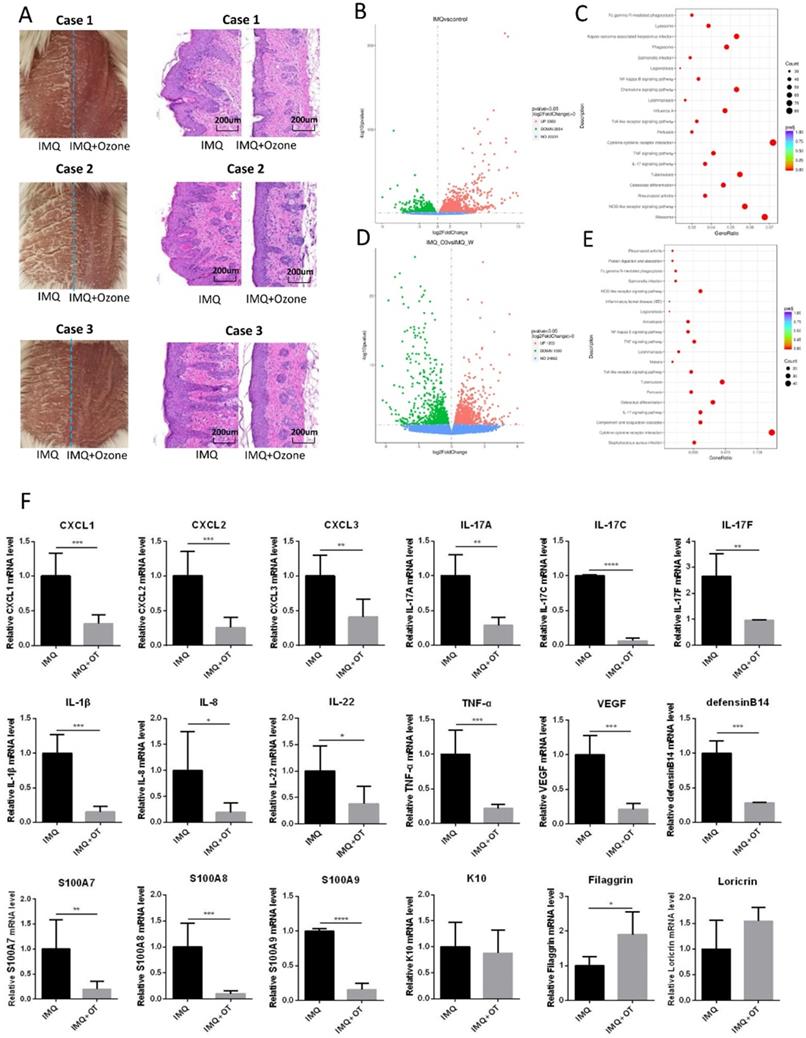{kind=link}
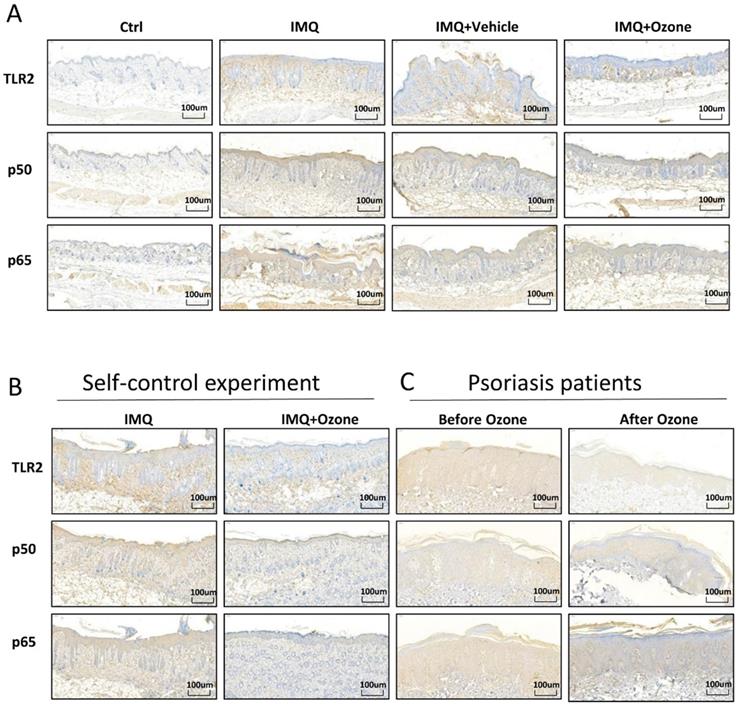{kind=link}
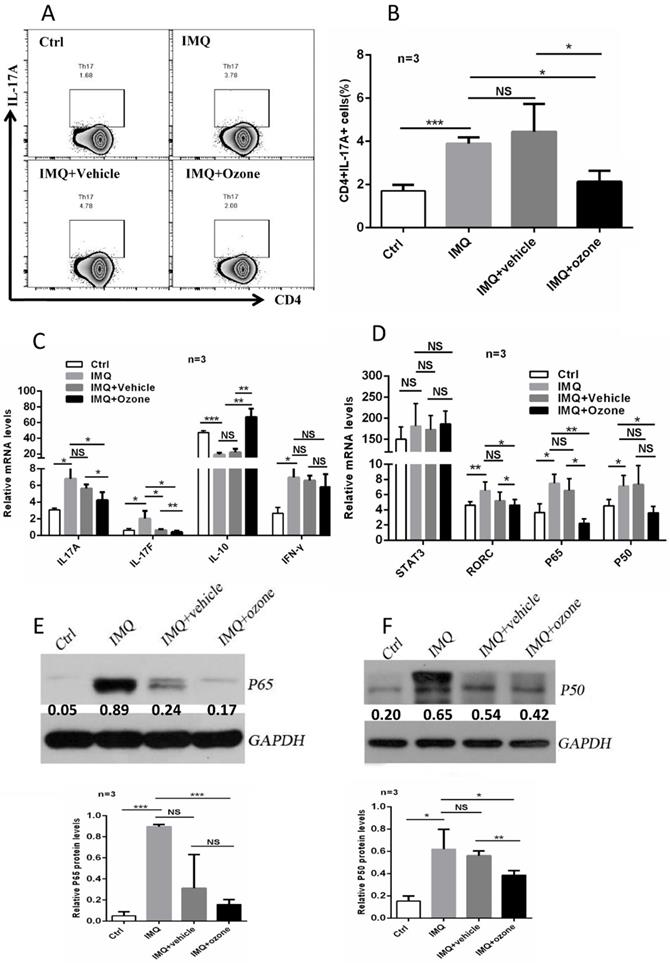{kind=link}