1. Department of Dermatology, Third Xiangya Hospital, Central South University, Changsha, Hunan, China;
2. XiangYa School of Medicine, Central South University, Changsha, Hunan, China;
3. Department of Cell Biology and Anatomy, School of Medicine, and
4. Department of Biomedical Engineering, College of Engineering and Computing, University of South Carolina, Columbia, South Carolina
*These authors contributed equally to this work.
✉ Corresponding author: Jianyun Lu, Department of Dermatology, Third Xiangya Hospital, Central South University, No. 138 Tongzipo Rd, Changsha, Hunan 410013, China. Telephone: +86-731-88618936. Fax: +86-731-88618936. Email: [email protected]
Citation:
Zeng J, Lei L, Zeng Q, Yao Y, Wu Y, Li Q, Gao L, Du H, Xie Y, Huang J, Tan W, Lu J. Ozone Therapy Attenuates NF-κB-Mediated Local Inflammatory Response and Activation of Th17 Cells in Treatment for Psoriasis. Int J Biol Sci 2020; 16(11):1833-1845. doi:10.7150/ijbs.41940. https://www.ijbs.com/v16p1833.htm
Ozone therapy has been widely used to treat many skin diseases, including infections, allergic dermatosis, and skin ulcers. However, its efficacy as a treatment for psoriasis is unclear. In this study, we explored the clinical efficacy and the underlying molecular mechanisms of ozone therapy on psoriasis. We found that topical ozone treatment significantly decreased patients' psoriasis area and severity index (PASI) scores and the expression of psoriasis-associated cytokines in their peripheral blood CD4+ T cells. In the IMQ-induced psoriasis mouse model, topical ozone treatment significantly inhibited the formation of IMQ-induced psoriasis-like lesions and the expression of psoriasis-associated inflammatory factors. High-throughput sequencing confirmed that IMQ-induced activation of toll-like receptor 2 (TLR2)/ nuclear factor-κB (NF-κB) signaling pathway was significantly suppressed in psoriasis-like lesions after topical ozone treatment. Furthermore, the activation of spleen T helper (Th) 17 cells was blocked in the mouse model; this was associated with the downregulation of cytokines and NF-κB pathways upon topical ozone treatment. Ozone therapy can attenuate local inflammatory reactions and the activation of Th17 cells in psoriasis by inhibiting the NF-κB pathway. Our results show that ozone therapy is effective in treating psoriasis. We recommend further evaluations for its clinical applications.
Psoriasis vulgaris is a long-lasting immune-mediated inflammatory cutaneous disease that is characterized by red, itchy, and scaly skin patches. Patients generally suffer disfiguration, disability, and associated comorbidities [1]. Environmental risk factors, such as microbial infections, obesity, and exposure to ultraviolet radiation, can trigger the onset of the disease in patients with latent psoriatic genetic susceptibility [2]. Plasmacytoid dendritic cells (pDCs) have been identified as inducers in the inflammatory cascade in psoriatic plaques [3]. Local pDCs in psoriatic skin lesions can activate and induce the differentiation of T helper (Th) cells into Th17, Th1, and Th22 subsets by producing IL-23, IL-12, IL-6, and tumor necrosis factor (TNF)-α [4, 5]. Evidence has shown that proportions of Th1 and Th17 cells in the skin lesions and peripheral blood of psoriatic patients are significantly increased as compared with normal subjects; Th2 cells and their associated cytokines; including IL-4, IL-10, and IL-13, show decreased proportions [6, 7]. Therefore, the blocking of pathogenic T cell activation, particularly the Th17 subset, has led to many remedies, such as assecukinumab [8], ixekizumab [9], and brodalumab [10]. However, problems related to biological agents, such as the single effect, high costs, and drug resistance, are major concerns to many patients and physicians. In addition, multiple inflammatory cytokine-stimulated NF-κB pathways are constitutively activated in psoriatic epidermis, resulting in hyperproliferation of keratinocytes [11, 12]. Activation of toll-like receptor 2 (TLR2) in keratinocytes can lead to the nuclear translocation of NF-κB and release of the proinflammatory cytokines TNF-α and IL-8 [13]. Microorganisms and their components and pathogen-associated molecular patterns (PAMPs) can trigger TLR2 to induce immune system activation [14]. Therefore, targeting the TLR2/NF-κB pathway is a potential novel therapeutic strategy.
Ozone was first applied clinically as a sterilizing agent due to its strong oxidizing property. It has been widely used to treat more than 50 different pathological conditions, including infectious skin diseases [15-18], allergic diseases [19, 20], erythema scaly diseases [21, 22], wound healing, and ulcer recovery [23]. The mechanisms of ozone's action may underlie antimicrobial effects, immunoregulation, antioxidant defenses, epigenetic modification, biosynthesis, analgesics, and vasodilation [24]. Current ozone medical preparations for dermatology fall into the following primary classifications: ozone hydrotherapy, topical ozonated oil, ozone autohemotherapy (OAHT), and ozone gas cavity/acupoint injection [24]. Recent studies have shown that a precise control of ozone concentrations can induce the production of various cytokines, such as IFN-γ, IL-6, and TNF-α [25]. Ozone can induce and activate the body's antioxidant enzyme system to produce free radical scavenging agents, remove some of the free radicals generated by inflammatory reactions, and interfere with the production of inflammatory factors during disease development [26]. However, the exact mechanisms of ozone therapy in treating diseases need to be further elucidated.
In this study, we evaluated the therapeutic efficacy of a short-term ozone treatment for psoriatic patients. We investigated potential mechanisms of topical ozone therapy for psoriasis using the imiquimod- (IMQ) induced psoriasis-like mouse model. We found that ozone therapy attenuated inflammatory responses in psoriasis by inhibiting the NF-κB pathway. Our results show that ozone therapy is a safe and effective treatment for psoriasis and is worthy of further clinical evaluations and applications.
Materials and Methods
Patients
This study was approved by the institutional review board (IRB) of the Third Xiangya Hospital, Central South University, Changsha, Hunan, China. A total of 10 psoriatic patients diagnosed with psoriasis vulgaris were enrolled in the study, and written consent forms were signed by all subjects. Clinical information on the patients is shown in Supplementary Table 1. PASI scores were used to assess disease activity. Study inclusion criteria were for patients between the ages of 18 and 60 years old and with psoriasis vulgaris diagnosed by pathologic examinations. Exclusion criteria included being allergic to ozonated water or oil; pregnancy or breastfeeding; severe systemic diseases; and having received corticosteroids, vitamin D3 derivatives, immune inhibitors, biological therapy, or oral retinoids within the previous 2 weeks.
Mice
The BALB/c mice were purchased from Hunan SJA Laboratory Animal Co., Ltd. At the age of 6 weeks, female mice were all adaptively fed for 1 week and used for all experiments. All animals were raised and handled in the animal experiment center of Central South University in strict accordance with relevant laws and institutional guidelines. All animal procedures were approved and supervised by the Medicine Animal Care and Use Committee of the Third Xiangya Hospital of Central South University.
Topical Ozone Therapy
All participants were treated with an ozonated water shower (3.0±1.5 mg/L, HZ-2601B, Hunan Health Care Technology, Changsha, China) for 15 minutes, once per day, then treated with topical ozonated oil (20160522, with an approximate peroxide value of 2,000-2,400 mmol-equivalent/kg, Hunan Health Care Technology, Changsha, China) twice per day, for 14 days.
Evaluation of Clinical Photographs and Reflectance Confocal Microscope Images of Skin Lesions
All subjects received free ozone therapy only; they did not receive any other treatments and drugs during the trial. The intervention lasted 14 days. Clinical photographs, PASI scores, and RCM images were assessed by the same professional physicians in order to score disease severity before and after treatments. PASI scores included the area of skin lesions, erythema, scaling, and thickening, according to the literature [27]. Each subject was assessed by RCM images from three different skin lesion sites. The total RCM scanned thickness of the skin was 51 layers × 3.05 µm (vertically) in each layer. Under RCM, epidermal thickness and infiltrated inflammatory cells were also evaluated prior to and post-treatment.
IMQ-Induced Mouse Model of Psoriasis and Ozone Intervention
Female BALB/c mice (aged 6-8 weeks) were fed under suitable conditions. The mice were smeared daily with a topical 5% IMQ cream (Sichuan Med-Shine Pharmaceutical Co., Ltd., H20030128, Sichuan, China) on their shaved dorsal skins for 7 consecutive days. Mice in the control group were treated with the same quantity of the vehicle cream. All IMQ mice were randomly divided into three groups: the nonintervention group (IMQ group), the ozone-treatment group (IMQ+Ozone), and the vehicle cream-treatment group (IMQ+Vehicle). The ozone-treatment group was treated with ozonated water (HZ-2601B, Hunan Health Care Technology Co., Ltd., Changsha, China) for 15 minutes once per day, then treated with topical ozonated oil (20160522, Hunan Health Care Technology Co., Ltd., Changsha, China). The vehicle cream-treatment group received tap water and base oil at the same frequency. The intervention lasted for 7 days. Clinical photographs and PASI scores were collected in order to evaluate the phenotypic characteristics. At the 7th day, all mice were sacrificed to collect skin lesions, spleen tissues, and lymph nodes.
Isolation of CD4+ T Cells
Peripheral blood mononuclear cells (PBMCs) were separated from peripheral blood of patients before and after treatment by centrifugation using a density gradient medium (GE Healthcare, Chicago, IL, USA). CD4+ T cells were isolated by a positive selection using Miltenyi beads according to the manufacturer's instructions (Miltenyi Biotec, Bergisch Gladbach, Germany). Next, the isolated CD4+ T cells were collected for subsequent experiments. In the mouse experiment, CD4+ T cells were purified from pooled single-cell suspensions of spleen using a mouse CD4+ T cell isolation kit from Miltenyi Biotec (Bergisch Gladbach, Germany).
Flow Cytometry
Surface markers, cytokines, and transcriptional factors were detected using an FACSCanto II cell analyzer (BD Biosciences, San Jose, CA, USA). For cytokine detection, isolated cells were stimulated in vitro for 4 h with phorbol 12-myristate 13-acetate (PMA) and ionomycin (Sigma-Aldrich, St. Louis, MO, USA) with the addition of GolgiPlug (BD Biosciences, San Jose, CA, USA) to promote the release of cytokines. Subsequently, the treated cells were incubated with antibodies against surface markers on ice for 30 min in the dark. For intracellular staining, cells were fixed and permeabilized with an eBioscience forkhead box P3 (FOXP3) transcription factor staining buffer set (catalog No. 00-5523, San Diego, CA, USA) and then stained with fluorescent antibodies for an additional 30 min on ice in the dark. Items were collected and analyzed using the FlowJo software (FlowJo LLC, Ashland, OR, USA). The following antibodies were obtained from BioLegend (San Diego, CA, USA) and used in this study: FITC anti-mouse IFN-γ (catalog No. 505805), Alexa Fluor 647 anti-mouse IL-17A (catalog No. 506911), PE anti-mouse IL-4 (catalog No. 504103), PE anti-mouse FOXP3 (catalog No. 126403), PerCP/Cy5.5 anti-mouse CD4 (catalog No. 100540), and FITC anti-mouse CD3 (catalog No. 5100203). Phycoerythrin (PE) anti-mouse IL-4 was obtained from BD Biosciences (catalog No. 504103, San Jose, CA, USA) and APC anti-mouse CD25 was obtained from eBioscience (catalog No. 102011, San Diego, CA, USA).
qPCR
Total RNA was extracted from cells or skin tissues using TRIzol according to the manufacturer's instructions (Thermo Fisher Scientific, Waltham, MA, USA). The mRNA was reverse-transcribed with the PrimeScript® RT reagent kit (Takara Biomedical Technology Co., Ltd., Kusatsu, Shiga, Japan) with 1 μg of total RNA in each reaction. The reaction mixture for real-time PCR contained 2 μL of cDNA, 10 μL of SYBR Premix Ex Taq™ (Takara Biomedical Technology Co., Ltd., Kusatsu, Shiga, Japan), and 400 nM of sense and antisense primers for a final volume of 20 μL. The qPCR was performed on a LightCycler® 96 (Roche, Rotkreuz, Switzerland) thermocycler. The quantity of gene expression was calculated using the 2-ΔCt methods and normalized to glyceraldehyde-3-phosphate dehydrogenase (GAPDH). Primers are shown in Supplementary Table 2.
Western Blotting
CD4+ T cells were lysated and proteins were extracted using a nuclear extraction reagent (Boster Biological Technology, Pleasanton, CA, USA). Proteins were quantified by the Bradford reagent (Thermo Fisher Scientific, Waltham, MA, USA), followed by 12% vertical dodecyl sulfate-polyacrylamide gel electrophoresis. Proteins were then transferred into a polyvinylidene difluoride (PVDF) membrane (Sigma-Aldrich, St. Louis, MO, USA). The PVDF membrane was blocked in 5% skim milk for 1 h at room temperature, then incubated with an antibody against P65 (GB11142, 1:1000, Wuhan Servicebio Technology Co., Ltd., Wuhan, China) or P50 (ab7971, 1:5000, Abcam, Cambridge, MA, USA) for 12-16 h at 4℃ , and followed by incubating with a mouse anti-rabbit IgG antibody (H&L) (GenScript, Piscataway, NJ, USA). Proteins were detected with an enhanced chemiluminescence (ECL) western blot detection kit (Thermo Fisher Scientific, Waltham, MA, USA). Quantification of P65 and P50 was normalized to GAPDH by densitometry.
Histological Analysis
Skin tissues from all patients and mice were fixed in formalin and embedded in paraffin (Wuhan Servicebio Technology Co., Ltd., Wuhan, China). Sections (6 µm) were stained with hematoxylin and eosin and stored at room temperature. Epidermal thickness and infiltrating inflammatory cells were assessed.
Immunohistochemical Staining
Sections (6 µm) were stained with P50 (catalog No. BS1249, Bioworld Technology Co., Ltd., Nanjing, China), P65 (catalog No. 10745-1-AP, Proteintech, Rosemont, IL, USA) and TLR2 antibodies (catalog No. ab213676, Abcam, Cambridge, MA, USA) according to the manufacturers' instructions. Image analysis was performed using a fluorescent microscope and Leica Qwin Std analysis software (Leica, Wetzlar, Germany).
High-Throughput Sequencing
Transcriptome profiles of the left and right sides of the skin lesions from self-control mouse models and lesions from the mouse dorsal skins in the control group and the IMQ group were obtained. Briefly, total RNA was extracted from these skin samples; the mRNA was enriched, fragmented and used for the cDNA synthesis. The cDNA fragments were amplified by PCR, and the size and quality of sequencing library were determined using an Agilent 2100 Bioanalyzer (Agilent, Santa Clara, CA, USA). The library was sequenced using a HiSeq X Ten high-throughput sequencing platform (Illumina Inc., San Diego, CA, USA). The differentially expressed genes among the selected samples were analyzed by Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analysis.
Statistical Analysis
All of the diagrams and graphs reporting cumulative data were generated using a GraphPad Prism 6.0 (GraphPad Software, San Diego, CA, USA). The data are represented as means ± standard error of the mean (SEM). Distributions of the means were analyzed with nonparametric tests (SPSS 18.0, IBM, Armonk, NY, USA). Differences in individual treatments were analyzed by paired t tests. Statistical significance (*P < 0.05, **P < 0.01, ***P < 0.001) was assessed using a 2-tailed unpaired Student t test for comparisons between 2 groups and 1-way analysis of variance (ANOVA) with relevant post hoc tests for multiple comparisons.
Results
Topical ozone treatment improves the condition of skin lesions in psoriasis
In order to evaluate the efficacy of ozone therapy on psoriasis, we enrolled ten patients with a diagnosis of psoriasis via cutaneous histopathology in this study. Each patient's psoriatic condition was determined using a psoriasis area and severity index (PASI) score, which was assessed four times over two weeks. In addition, clinical photographs, reflectance confocal microscopy (RCM), and hematoxylin and eosin (HE) staining were used to evaluate each patient's pathological characteristics before and after treatment. The patients' psoriatic skin lesions improved significantly after ozone therapy; clinical and histological improvements were evident in patients (Figure 1a and b). There were obvious attenuations of inflammatory erythema and scales showing in clinical photographs (Figure 1a). Histology and RCM images showed that the epidermis was significantly thinner and that infiltrating inflammatory cells had decreased after 14 days ozone treatment as compared to before treatment (Figure 1b-d). Correspondingly, the PASI scores dropped significantly after the 14-day treatment as compared with baselines (Figure 1e). In order to investigate the potential mechanisms of ozone action on psoriasis, we assessed the expression levels of common psoriatic-associated cytokines and transcription factors in CD4+ T cells from the patients' peripheral blood using quantitative real-time PCR (qPCR). Being expected, the expression levels of IL-17a, IL-6, TNF-α, transforming growth factor (TGF)-β, IFN-γ, and NF-κB were down-regulated after ozone-treatment as compared with prior to treatment (Figure 1f). The expression levels of IL-17f and the Th17-cell-specific transcription factor retinoid-related orphan nuclear receptor c (RORc) decreased after ozone treatment, but the decrease had no statistical significance (Figure 1f). The expression of IL-10 increased after ozone treatment, but not significantly. These results were consistent with the clinical efficacy. Taken together, our results demonstrate that topical ozone treatment can improve the condition of psoriatic skin lesions in patients by an inhibition of inflammatory processes.
Figure 1Topical ozone treatment improves the pathological conditions of psoriatic skin lesions. (a) Clinical photographs of a psoriatic skin lesion on days 0 (D0) and 14 (D14) with an ozone therapy. (b) HE staining of psoriatic skin lesion before and after treatment. (c) Evaluation of RCM images showing the 25th and 50th scanning layers before and after treatment. (d) Statistical analysis of vertical swept layers of quantitative RCM images for an assessment of thickness of epidermis; (e) PASI scores for all participants. (f) Quantitative PCR to detect expression levels of cytokines and transcriptional factors in CD4+ T cells from peripheral blood of psoriasis patients before and after treatment. Note: * = P < 0.05; ** = P < 0.01; *** = P < 0.001; NS = no statistical significance.
Inhibition of IMQ-induced psoriasis-like phenotypes by topical ozone treatment
In order to further evaluate the therapeutic efficacy of topical ozone on psoriasis, we used IMQ to induce psoriasis-like lesions on dorsal skins of BALB/c mice [28]. Daily application of topical ozone resulted in a significant inhibition of IMQ-induced psoriasis-like lesions as compared to the vehicle-treatment group (water + base oil) (Figure 2a). The topical ozone treatment prevented IMQ-induced weight loss (Figure 2b) and improved PASI scores (Figure 2c) in the IMQ-induced psoriatic mice. Previous studies [6] have shown that IMQ can cause enlargement of the spleen in this mouse model. We found that topical ozone treatment resulted in a significant inhibition of the increased spleen-to-body-weight ratio as compared with the no-treatment or vehicle-treatment groups (Figure 2d). These results demonstrate that topical ozone treatment can inhibit IMQ-induced psoriasis-like phenotypes in this mouse model.
Inhibition of IMQ-induced psoriasis-like inflammation by topical ozone treatment
In order to further investigate the mechanism underlying topical ozone treatment for IMQ-induced psoriasis-like lesions, we treated the right side of each lesion with topical ozone and kept the left side of the lesion untreated as a contralateral control (Figure 3a). We analyzed transcriptomes in the skin lesions after ozone treatment by RNA sequencing (RNA-seq) and compared with the skin lesions without treatment. We found that IMQ caused an increase in expression of 3083 genes and decrease in expression of 2854 genes, respectively, as compared with the control (Figure 3b). KEGG pathway enrichment analysis revealed that the inflammatory-related signaling pathways such as NF-κB, TLR, TNF, and IL-17 were significantly activated in the IMQ-induced psoriasis mouse model (Figure 3c). In contrast, topical ozone treatment (right side of the lesion) increased expression levels of 1023 genes and decreased expression levels of 1000 genes, respectively, as compared to the lesions without treatment (the left side of the lesions) (Figure 3d). Interestingly, IMQ-induced activation of NF-κB, TLR, TNF, and IL-17 signaling pathways was significantly inhibited by topical ozone application (Figure 3e). Further quantitative RT-PCR confirmed that topical ozone therapy could significantly inhibit the expression of many chemokines, such as C-X-C motif ligand (CXCL) 1, CXCL2, and CXCL3, and psoriasis-associated inflammatory factors, including IL-17a, IL-17c, IL-17f, IL-1β, IL-8, IL-22, TNF-α, vascular endothelial growth factor (VEGF), defensin B14, S100A7, S100A8, and S100A9 (Figure 3f). These results demonstrate that topical ozone therapy can treat psoriasis lesions via inhibition of the local inflammatory processes.
Inhibition of TLR2/NF-κB signaling by topical ozone treatment
Many studies have shown that the TLR2/NF-κB signaling pathway promotes the release of multiple inflammatory factors in psoriasis lesions, aggravating the inflammatory response of psoriasis lesions. In order to examine whether topical ozone could inhibit TLR2/NF-κB signaling, we used immunohistochemistry to characterize the expression profiles of TLR2, P50, and P65 in IMQ-induced psoriasis-like lesions and in patients. We found that topical ozone treatment significantly decreased the IMQ-induced expression levels of TLR2, P50, and P65 in the mouse model (Figure 4a and b) and in patients with psoriasis (Figure 4c). Therefore, topical ozone treatment can significantly inhibit TLR2/NF-κB signaling in psoriatic skin lesions.
Suppression of Th17 differentiation by topical ozone treatment
Immune imbalance of CD4+ T subset is considered to be a critical factor in the pathogenesis of psoriasis. Evidence has shown that the PASI scores of psoriasis patients are positively related to IL-17 levels in serum and that Th17 cells are the main infiltrating T subset in psoriatic skin lesions [29]. Not surprising, ozone therapy resulted in a significant suppression of the IMQ-induced polarized Th17-cell proportions (Figure 5a and b). Ozone treatment significantly inhibited expression levels of T helper lymphocyte-associated cytokines (Figure 5c), including IL-17a, IL-17f, IL-10, and IFN-γ, and key transcription factors (Figure 5d), such as signal transducer and activator of transcription (STAT) 3, RORc, and NF-κB. Ultimately, we examined the expression levels of P50 and P65 in splenic CD4+ T cells among the four groups using western blotting. We found that ozone treatment significantly inhibited the expression of NF-κB (Figure 5e and f). Therefore, topical ozone therapy may suppress the IMQ-induced activation of RORc and NF-κB signaling pathways to regulate the differentiation of Th17 cells. Moreover, we also assessed the differentiated proportions of Th1 cells, Th2 cells, and regulatory T (Treg) cells. There was no significant effect on the levels of Th1 and Th2 cells; the proportion of Treg cells was upregulated slightly (Supplementary Figure 1a-c). These data demonstrate that ozone may act on psoriasis mainly by inhibiting the activation and proliferation of Th17 cells and expression of their associated cytokines.
Figure 2Topical ozone treatment significantly inhibits IMQ-induced psoriasis-like lesions in mouse skin. Mice were randomly divided into four groups: Ctrl, IMQ, IMQ+Vehicle, and IMQ+Ozone. (a) The skin lesions and histological features among different treatment groups. (b) Changes of body weight and (c) PASI scores for mice in different treatment groups. (d) Spleen and spleen-to-body-weight ratio in different treatment groups. Note: * = P < 0.05; ** = P < 0.01; *** = P < 0.001; NS = no statistical significance.
Figure 3Topical ozone treatment significantly inhibits IMQ-induced psoriasis- like inflammation. (a) Psoriasis-like lesions were induced on dorsal skins of mice using IMQ. Topical ozone cream was applied on the right side of the lesion but not on the left side of the lesion. (b) Transcriptome analysis showing that IMQ induced an upregulation and downregulation of expression levels of 3063 and 2854 genes, respectively, in lesions as compared with normal skin. (c) Enrichment of the upregulated KEGG signaling pathway in the IMQ group versus control group. (d) Transcriptome analysis showing that ozone treatment caused an upregulation and downregulation of expression levels of 1203 and 1000 genes, respectively, in lesions as compared with IMQ induction group in the self-control experiment. (e) Enrichment of downregulated KEGG signaling pathway in the IMQ+Ozone group versus IMQ group. (f) Validation of changes in various psoriasis-associated inflammatory factors using qPCR. Note: * = P < 0.05; ** = P < 0.01; *** = P < 0.001; NS = no statistical significance.
Figure 4Topical ozone treatment significantly inhibits TLR2/NF-κB signaling. (a) Expression levels of TLR2, P50, and P65 in skin lesions from Ctrl, IMQ, IMQ+Vehicle, and IMQ+Ozone groups were evaluated by immunohistochemical analysis. (b) Expression levels of TLR2, P50, and P65 in IMQ-induced self-control mouse skin lesions and (c) human psoriasis lesions before and after ozone treatment.
High concentrations of ozone can induce cell damage, leading to respiratory diseases, headaches, skin irritation, and so forth [30-32]. However, low concentrations of ozone in the therapeutic range (10-80 μg/ml of gas) can be effectively quenched by the body's powerful antioxidative capacity in order to avoid toxic effects on cells; such concentrations of ozone have been used as a sterilizing agent, promote wound healing, regulate immunity, and carried out analgesic functions [33]. Ozone can quickly produce oxygen, reactive oxygen species (ROS), lipid oxidation products (LOPs), and aldehydes when in contact with skin tissue. ROS function as short-acting messengers and quickly disappear; LOPs can enter the blood circulation through lymphatic vessels and capillaries, and function as long-acting messengers. Aldehydes combine with cysteine and glutathione (GSH) to form a stable olefin adduct that can enter various cells of the human body, activating the nuclear factor erythroid 2-related factor 2 (Nrf2)- antioxidant response element (ARE) signaling pathway to improve antioxidant capacity [33]. Ozone can play a therapeutic role in many inflammatory diseases due to its antioxidant capacity. For instance, ozone therapy ameliorates inflammation and endometrial injury in rats with pelvic inflammatory diseases [34]. Local ozone therapy inhibits the expression of inflammatory factors such as pentraxin-3 (PTX-3), IL-1β, and high-sensitivity C-reactive protein (Hs-CRP) in periodontitis patients [35]. We have shown that local ozone therapy not only can kill Staphylococcus aureus in atopic dermatitis but also can inhibit inflammation by inhibiting the expression of IL-4 [36, 37]. An increasing body of evidence suggests that ozone therapy may be able to replace or reduce clinical usages of antibiotics and glucocorticoids, thereby decreasing risks such as antibiotic resistance and side effects from the long-term use of glucocorticoids.
Figure 5Topical ozone treatment suppresses Th17 differentiation to mitigate psoriasis disease. (a) Flow cytometry to determine the proportion of Th17 cells in mouse spleens and lymph nodes from four groups, e.g. Ctrl, IMQ, IMQ+Vehicle, and IMQ+Ozone. (b) Statistical analysis of the proportion of Th17 cells among different groups. Quantitative PCR to examine expression levels of cytokines (c) and transcriptional factors (d) in CD4+ T cells isolated from mouse spleens and lymph nodes. Western blotting to evaluate expression levels of P65 (d) and P50 (e) in CD4+ T cells isolated from mouse spleens and lymph nodes from four groups. The relative expression levels were normalized to GAPDH levels. Note: * = P < 0.05; ** = P < 0.01; *** = P < 0.001; NS = no statistical significance.
Psoriasis is a chronic relapsing inflammatory skin disease. We posit that ozone therapy can control the progression of psoriasis by inhibiting the inflammatory response of skin lesions. Studies have found that ozonated oil not only delivers reactive oxygen but also maintains therapeutically active ozonated derivatives for a long time [38]. Our previous studies have found that ozonated oil is safe and effective for the treatment of stable psoriasis vulgaris, with an efficacy equivalent to that of intermediate-acting glucocorticoids [39]. In this study, we have demonstrated that patients' psoriatic skin lesions are mitigated significantly and that inflammatory biomarkers such as IL-17a, IL-6, TNF-α, TGF-β, and IFN-γ are downregulated significantly after ozone treatment. We have also shown that ozone therapy can significantly inhibit inflammatory-related pathways, such as NF-κB, TLR, TNF, and IL-17, in a psoriasis animal model. These data provide an insight into the mechanisms underlying the therapeutic effects of ozone therapy on psoriatic lesions.
Multiple studies have found elevated levels of TLRs in psoriatic lesions [40-43]. TLRs are a very important class of pattern recognition receptors (PRRs). After recognizing PAMPs, such as lipopolysaccharides, peptidoglycan, viral products, and bacterial nucleus components, TLRs activate downstream signaling pathways to induce innate immune activation by promoting the release of proinflammatory cytokines and initiating specific immune responses [44-46]. Abnormally increased PAMPs (such as lipopolysaccharides and peptidoglycan) in psoriatic lesions activate the NF-κB signaling pathway, promoting the expression of proinflammatory cytokines, which induces a strong inflammatory response in local psoriasis [47, 48]. In this study, we have shown that ozone treatment can significantly inhibit the TLR2/NF-κB signaling pathway in psoriatic lesions, thereby attenuating the local inflammatory response of psoriasis. There are a few potential explanations for this. First, ozone therapy can reduce the production of PAMPs by inhibiting colonized microorganisms on the surface of lesions, which reduces the activation of the TLR2/NF-κB pathway. Second, activation of the antioxidant system by ozone such as Nrf2-ARE in the body can antagonize the NF-κB-mediated inflammatory responses [49, 50]. Third, oxygen produced by ozone therapy can improve the hypoxic environment of psoriatic skin lesions and inhibit hypoxia-induced inflammatory responses.
The activation of Th17 cells is crucial for the inflammatory response of psoriasis vulgaris lesions [51]. Our results show that ozone treatment can significantly inhibit IMQ-induced increases in the number and active function of Th17 cells. Activation of the NF-κB signaling pathway can induce the activation of Th17 cells [52]. Therefore, ozone-mediated suppression of the activation of Th17 cells is probably due to the inhibition of NF-κB pathways. In addition to Th17 cells, other immune cells, such as Th1, Th2, dendritic cells (DCs), natural killer (NK) cells, and macrophages, are also involved in the inflammatory response of psoriasis [53]. However, our results show that ozone treatment has a minimal effect on these cells. Therefore, ozone likely has a specific effect on the regulation of Th17 cells during the treatment of psoriasis.
In addition to ozonated water and oil, ozone autohemotherapy and ozone gas cavity/acupoint injection have also been reported to improve the body's antioxidant capacity and regulate inflammation [54-56]. Whether these treatments can be used for psoriasis has yet to be determined. Ozone can also be used in combination with other agents in order to reduce side effects and increase efficacy. For example, combined intradiscal and periganglionic injection of medical ozone and steroids has a cumulative effect, leading to enhanced overall outcomes in the treatment of pain caused by disk herniation [57]. Local ozone therapy has a few side effects, such as irritating pain. It rarely produces systemic side effects. There are some limitations in this study. For example, there are no data regarding the long-term efficacy of the treatment or its impact on recurrence rates. The question of whether ozone treatment plays a regulatory role in the proliferation and differentiation of keratinocytes and in the vasodilation of psoriasis has not yet been answered.
This work was supported by the New Xiangya Talent Projects of the Third Xiangya Hospital of Central South University (Grant No. 20170309) and National Undergraduate Innovation Training Program of Central South University (Grant No. GS201910533570).
Competing Interests
The authors have declared that no competing interest exists.
References
1. Boehncke WH, Schon MP. Psoriasis. Lancet. 2015;386:983-94
2. Zeng J, Luo S, Huang Y, Lu Q. Critical role of environmental factors in the pathogenesis of psoriasis. The Journal of dermatology. 2017;44:863-72
3. Becher B, Pantelyushin S. Hiding under the skin: Interleukin-17-producing gammadelta T cells go under the skin?. Nature medicine. 2012;18:1748-50
4. Krueger JG. Hiding under the skin: A welcome surprise in psoriasis. Nature medicine. 2012;18:1750-1
5. Gutcher I, Becher B. APC-derived cytokines and T cell polarization in autoimmune inflammation. The Journal of clinical investigation. 2007;117:1119-27
6. Wu R, Zeng J, Yuan J, Deng X, Huang Y, Chen L. et al. MicroRNA-210 overexpression promotes psoriasis-like inflammation by inducing Th1 and Th17 cell differentiation. The Journal of clinical investigation. 2018;128:2551-68
7. Kagami S, Rizzo HL, Lee JJ, Koguchi Y, Blauvelt A. Circulating Th17, Th22, and Th1 cells are increased in psoriasis. The Journal of investigative dermatology. 2010;130:1373-83
8. Speeckaert R, van Geel N, Lambert J, Claeys L, Delanghe JR, Speeckaert MM. Secukinumab: IL-17A inhibition to treat psoriatic arthritis. Drugs of today (Barcelona, Spain: 1998). 2016;52:607-16
9. Toussirot E. Ixekizumab: an anti- IL-17A monoclonal antibody for the treatment of psoriatic arthritis. Expert opinion on biological therapy. 2018;18:101-7
10. Lebwohl MG, Papp KA, Marangell LB, Koo J, Blauvelt A, Gooderham M. et al. Psychiatric adverse events during treatment with brodalumab: Analysis of psoriasis clinical trials. Journal of the American Academy of Dermatology. 2018;78:81-9.e5
11. Yan S, Xu Z, Lou F, Zhang L, Ke F, Bai J. et al. NF-kappaB-induced microRNA-31 promotes epidermal hyperplasia by repressing protein phosphatase 6 in psoriasis. Nature communications. 2015;6:7652
12. Hara-Chikuma M, Satooka H, Watanabe S, Honda T, Miyachi Y, Watanabe T. et al. Aquaporin-3-mediated hydrogen peroxide transport is required for NF-kappaB signalling in keratinocytes and development of psoriasis. Nature communications. 2015;6:7454
13. Begon E, Michel L, Flageul B, Beaudoin I, Jean-Louis F, Bachelez H. et al. Expression, subcellular localization and cytokinic modulation of Toll-like receptors (TLRs) in normal human keratinocytes: TLR2 up-regulation in psoriatic skin. European journal of dermatology: EJD. 2007;17:497-506
14. Choudhary V, Uaratanawong R, Patel RR, Patel H, Bao W, Hartney B. et al. Phosphatidylglycerol Inhibits Toll-Like Receptor-Mediated Inflammation by Danger-Associated Molecular Patterns. The Journal of investigative dermatology. 2019;139:868-77
15. Bialoszewski D, Pietruczuk-Padzik A, Kalicinska A, Bocian E, Czajkowska M, Bukowska B. et al. Activity of ozonated water and ozone against Staphylococcus aureus and Pseudomonas aeruginosa biofilms. Medical science monitor: international medical journal of experimental and clinical research. 2011;17:Br339-44
16. Zanardi I, Burgassi S, Paccagnini E, Gentile M, Bocci V, Travagli V. What is the best strategy for enhancing the effects of topically applied ozonated oils in cutaneous infections?. BioMed research international. 2013;2013:702949
17. Ouf SA, Moussa TA, Abd-Elmegeed AM, Eltahlawy SR. Anti-fungal potential of ozone against some dermatophytes. Brazilian journal of microbiology: [publication of the Brazilian Society for Microbiology]. 2016;47:697-702
18. Jenerowicz D, Silny W, Danczak-Pazdrowska A, Polanska A, Osmola-Mankowska A, Olek-Hrab K. Environmental factors and allergic diseases. Annals of agricultural and environmental medicine: AAEM. 2012;19:475-81
19. Gershwin LJ. Comparative immunology of allergic responses. Annual review of animal biosciences. 2015;3:327-46
20. Di Paolo N, Gaggiotti E, Galli F. Extracorporeal blood oxygenation and ozonation: clinical and biological implications of ozone therapy. Redox report: communications in free radical research. 2005;10:121-30
21. Bocci V, Zanardia I, Valacchi G, Borrelli E, Travagli V. Validity of Oxygen-Ozone Therapy as Integrated Medication Form in Chronic Inflammatory Diseases. Cardiovascular & hematological disorders drug targets. 2015;15:127-38
22. Polydorou O, Halili A, Wittmer A, Pelz K, Hahn P. The antibacterial effect of gas ozone after 2 months of in vitro evaluation. Clinical oral investigations. 2012;16:545-50
23. Borges GA, Elias ST, da Silva SM, Magalhaes PO, Macedo SB, Ribeiro AP. et al. In vitro evaluation of wound healing and antimicrobial potential of ozone therapy. Journal of cranio-maxillo-facial surgery: official publication of the European Association for Cranio-Maxillo-Facial Surgery. 2017;45:364-70
24. Zeng J, Lu J. Mechanisms of action involved in ozone-therapy in skin diseases. International immunopharmacology. 2018;56:235-41
25. Wu D, Tan W, Zhang Q, Zhang X, Song H. Effects of ozone exposure mediated by BEAS-2B cells on T cells activation: a possible link between environment and asthma. Asian Pacific journal of allergy and immunology. 2014;32:25-33
26. Delgado-Roche L, Martinez-Sanchez G, Re L. Ozone oxidative preconditioning prevents atherosclerosis development in New Zealand White rabbits. Journal of cardiovascular pharmacology. 2013;61:160-5
27. Reich K, Gooderham M, Thaci D, Crowley JJ, Ryan C, Krueger JG. et al. Risankizumab compared with adalimumab in patients with moderate-to-severe plaque psoriasis (IMMvent): a randomised, double-blind, active-comparator-controlled phase 3 trial. Lancet. 2019;394:576-586
28. van der Fits L, Mourits S, Voerman JS, Kant M, Boon L, Laman JD. et al. Imiquimod-induced psoriasis-like skin inflammation in mice is mediated via the IL-23/IL-17 axis. Journal of immunology. 2009;182:5836-45
29. van der Fits L, Mourits S, Voerman JS, Kant M, Boon L, Laman JD. et al. Imiquimod-induced psoriasis-like skin inflammation in mice is mediated via the IL-23/IL-17 axis. Journal of immunology (Baltimore, Md: 1950). 2009;182:5836-45
30. English P, Balmes J. Associations between Ozone and Fine Particulate Matter and Respiratory Illness Found to Vary between Children and Adults. Implications for U.S. Air Quality Policy. American journal of respiratory and critical care medicine. 2019;199:817-9
31. Apte MG, Buchanan IS, Mendell MJ. Outdoor ozone and building-related symptoms in the BASE study. Indoor air. 2008;18:156-70
32. Balmes JR. Long-term Exposure to Ozone and Cardiopulmonary Mortality: Epidemiology Strikes Again. American journal of respiratory and critical care medicine. 2019;200:958-959
33. Bocci V, Di Paolo N. Oxygen-ozone therapy in medicine: an update. Blood purification. 2009;28:373-6
34. Wei A, Feng H, Jia XM, Tang H, Liao YY, Li BR. Ozone therapy ameliorates inflammation and endometrial injury in rats with pelvic inflammatory disease. Biomedicine & pharmacotherapy = Biomedecine & pharmacotherapie. 2018;107:1418-25
35. Tasdemir Z, Oskaybas MN, Alkan AB, Cakmak O. The effects of ozone therapy on periodontal therapy: A randomized placebo-controlled clinical trial. Oral diseases. 2019;25:1195-202
36. Qin G, Huang J, Pan Y, Xiang Y, Ou C, Huang J. et al. [Topical ozone application: An innovative therapy for infantile atopic dermatitis]. Zhong nan da xue xue bao Yi xue ban. 2018;43:163-7
37. Lu J, Li M, Huang J, Gao L, Pan Y, Fu Z. et al. [Effect of ozone on Staphylococcus aureus colonization in patients with atopic dermatitis]. Zhong nan da xue xue bao Yi xue ban. 2018;43:157-62
38. Travagli V, Zanardi I, Valacchi G, Bocci V. Ozone and ozonated oils in skin diseases: a review. Mediators of inflammation. 2010;2010:610418
39. Tan L, Huang J, Lu J, Lu J. [Clinical efficacy of ozonated oil in the treatment of psoriasis vulgaris]. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2018;43:173-8
40. Liu Y, Yin H, Zhao M, Lu Q. TLR2 and TLR4 in autoimmune diseases: a comprehensive review. Clinical reviews in allergy & immunology. 2014;47:136-47
41. Begon E, Michel L, Flageul B, Beaudoin I, Jean-Louis F, Bachelez H. et al. Expression, subcellular localization and cytokinic modulation of Toll-like receptors (TLRs) in normal human keratinocytes: TLR2 up-regulation in psoriatic skin. European journal of dermatology: EJD. 2007;17:497-506
42. Candia L, Marquez J, Hernandez C, Zea AH, Espinoza LR. Toll-like receptor-2 expression is upregulated in antigen-presenting cells from patients with psoriatic arthritis: a pathogenic role for innate immunity?. The Journal of rheumatology. 2007;34:374-9
43. Shao S, Fang H, Dang E, Xue K, Zhang J, Li B. et al. Neutrophil Extracellular Traps Promote Inflammatory Responses in Psoriasis via Activating Epidermal TLR4/IL-36R Crosstalk. Frontiers in immunology. 2019;10:746
44. Kay E, Scotland RS, Whiteford JR. Toll-like receptors: Role in inflammation and therapeutic potential. BioFactors (Oxford, England). 2014;40:284-94
45. Mahla RS, Reddy MC, Prasad DV, Kumar H. Sweeten PAMPs: Role of Sugar Complexed PAMPs in Innate Immunity and Vaccine Biology. Frontiers in immunology. 2013;4:248
46. Brown J, Wang H, Hajishengallis GN, Martin M. TLR-signaling networks: an integration of adaptor molecules, kinases, and cross-talk. Journal of dental research. 2011;90:417-27
47. Lee JH, Moon JH, Lee YJ, Park SY. SIRT1, a Class III Histone Deacetylase, Regulates LPS-Induced Inflammation in Human Keratinocytes and Mediates the Anti-Inflammatory Effects of Hinokitiol. The Journal of investigative dermatology. 2017;137:1257-66
48. Chen JQ, Szodoray P, Zeher M. Toll-Like Receptor Pathways in Autoimmune Diseases. Clinical reviews in allergy & immunology. 2016;50:1-17
49. Lu MC, Zhao J, Liu YT, Liu T, Tao MM, You QD. et al. CPUY192018, a potent inhibitor of the Keap1-Nrf2 protein-protein interaction, alleviates renal inflammation in mice by restricting oxidative stress and NF-κB activation. Redox biology. 2019;26:101266
50. Subedi L, Lee JH, Yumnam S, Ji E, Kim SY. Anti-Inflammatory Effect of Sulforaphane on LPS-Activated Microglia Potentially through JNK/AP-1/NF-κB Inhibition and Nrf2/HO-1 Activation. Cells. 2019;8:pii E194
51. Visvanathan S, Baum P, Vinisko R, Schmid R, Flack M, Lalovic B. et al. Psoriatic skin molecular and histopathologic profiles after treatment with risankizumab versus ustekinumab. The Journal of allergy and clinical immunology. 2019;143:2158-69
52. Zhou F, Zhu Z, Gao J, Yang C, Wen L, Liu L. et al. NFKB1 mediates Th1/Th17 activation in the pathogenesis of psoriasis. Cellular immunology. 2018;331:16-21
53. Deng Y, Chang C, Lu Q. The Inflammatory Response in Psoriasis: a Comprehensive Review. Clinical reviews in allergy & immunology. 2016;50:377-89
54. Sancak EB, Turkon H, Cukur S, Erimsah S, Akbas A, Gulpinar MT. et al. Major Ozonated Autohemotherapy Preconditioning Ameliorates Kidney Ischemia-Reperfusion Injury. Inflammation. 2016;39:209-17
55. Deng L, Meng W, Li D, Qiu D, Wang S, Liu H. The effect of ozone on hypoxia, hemolysis and morphological change of blood from patients with aortic dissection (AD): a preliminary experiment of ozonated autohemotherapy for treating AD. American journal of translational research. 2018;10:1829-40
56. Chen H, Yu B, Lu C, Lin Q. The effect of intra-articular injection of different concentrations of ozone on the level of TNF-α, TNF-R1, and TNF-R2 in rats with rheumatoid arthritis. Rheumatology international. 2013;33:1223-7
57. Andreula CF, Simonetti L, De Santis F, Agati R, Ricci R, Leonardi M. Minimally invasive oxygen-ozone therapy for lumbar disk herniation. AJNR American journal of neuroradiology. 2003;24:996-1000
Updated Review on Ozone Therapy in Pain Medicine
Francisco Javier Hidalgo-Tallón1*Luis Miguel Torres-Morera2Jose Baeza-Noci3Maria Dolores Carrillo-Izquierdo4Rosa Pinto-Bonilla3
1Institute of Neurosciences, University of Granada, Granada, Spain
2Department of Anesthesia, Resuscitation, and Pain Treatment Service, Hospital Puerta del Mar, Cadiz, Spain
3Department of Embryology and Human Anatomy, School of Medicine, University of Valencia, Valencia, Spain
4School of Nursing, Catholic University of Murcia (UCAM), Murcia, Spain
The use of medical ozone in the treatment of chronic pain is progressively expanding in Spain and today it is used both in public and private medical centers. However, there is a great lack of knowledge about this technology not only in primary care but also in medical specialties. Although its biochemical bases are well determined and there are various systematic reviews and meta-analyses in the literature that justify its use in pain medicine, some professionals still are prejudiced against it. The evidence level of using medical ozone according SIGN (Scotish Intercollegiate Guideline Network) criteria is similar or superior to most of the techniques used in a Pain Unit. In this paper, we have done a review on ozone therapy in pain medicine, compiling the evidence published about it.
Introduction
Ozone therapy is the use of medical ozone as a therapeutic substance in pathologies with chronic hypoxia, inflammation, and redox imbalance in which ozone has proven to be effective (Baeza et al., 2015). Medical ozone is a mixture of oxygen and ozone obtained from medical oxygen by using a medical device – a medical ozone generator approved by a Notified Body according to the European Directive 93/42 and national regulations (Spanish RD 1591/2009). Medical ozone generators for parenteral use are classified in heading IIB of the classification of medical devices in EU regulations. Ozone therapy in medicine is a growing reality, and there are more and more professionals using medical ozone as a therapeutic tool for different diseases related to chronic oxidative stress and inflammation, including chronic pain.
In addition to health professional associations (such as the Spanish Ozone Therapy Association—SEOT or the World Federation of Ozone Therapy—WFOT) that try to unify criteria and develop protocols of treatment, as well as training health professionals in the use of this substance, the Catholic University of Murcia has taken the initiative by creating a chair of Ozone Therapy and Chronic Pain to better promote training and researching inside the Spanish universities network.
In Portugal and Greece, ozone therapy has a specific regulation and is used in public and private centers. In the rest of the European Union, it is used thanks to the legal recognition of medical ozone generators. In 2011, the Spanish Ministry of Health included the ozone therapy in the portfolio of services of the pain units (Palanca-Sánchez et al., 2011), so it is necessary that doctors who are experts in pain management know the rationale of medical ozone therapy and how it works, both locally and systemically.
Ozone is a molecule composed of three oxygen atoms (O3) instead of the two oxygen atoms found in the oxygen molecule (O2). Ozone has a half-life of 40 min at 20°C (Baeza et al., 2015); for this reason, it cannot be stored and must be produced “in situ” for each application.
Medical ozone applications date back to the beginning of the last century. The papers compiled in this publication have been published in the last 25 years and the oldest one have been included for historic reasons. Dr. Kellogg, in his book on diphtheria (1881) already mentioned ozone as a disinfectant, and in 1898 Drs Thauerkauf and Luth founded in Berlin the “Institute for oxygen therapy,” carrying out the first trials with animals. In 1911, the book “A Working Manual of High-Frequency Currents”, published by Dr. Noble Eberhart, head of the department of physiological therapeutics at Loyola University, described the use of medical ozone in the treatment of diseases such as tuberculosis, anemia, asthma, bronchitis, hay fever, diabetes, etc. (Pressman, 2021). But despite the successes achieved at the beginning of the last century, the ozone generating machines lacked precision and were quite fragile as they used a lot of glass tubes.
When applying this therapy, we are really inducing a controlled and harmless “micro-oxidation” that will produce a modulation of the cellular antioxidant system and the inflammation system. Ozone reacts with interstitial fluids producing hydrogen peroxide (H2O2), aldehydes, and lipid oxidation products (LOPs). These substances induce activation of the nuclear factor erythroid 2-related factor 2 (NRF2) pathway that will induce an increase in antioxidant systems (ARE), such as superoxide dismutase (SOD), catalase (CAT), reduced glutathione (GSH), glutathione peroxidase (GSH-Px), glutathione s-tranferase (GSTr), hem-oxygenase-1 (HO-1), reduced nicotinamide adenine dinucleotide phosphate (NADPH), NADPH quinone oxidoreductase 1 (NQO1) and heat shock protein-70 (HSP70; Baeza et al., 2015). This NRF2 activation (Figure 1) induces a decrease in the nuclear factor kappa beta (NFKβ) pathway activity, inducing an anti-inflammatory effect [decrease of interleukynes 1,2,6,7 and tumor necrosis factor alpha (TNFα) and increase of interlukynes 4, 10, 13 and transforming growing factor beta (TGFβ)] In the injected tissues, medical ozone inactivates proteolytic enzymes through the inhibition of the NFKβ pathway. At the same time, there is a proliferation of fibroblasts and chondrocytes, favoring cartilaginous regeneration (Fernández-Cuadros et al., 2020).
figure 1
FIGURE 1. The chemical reaction between ozone and PUFA (poli-unsaturated fatty acids) in the insterstitial water (or plasma) produce several ROS, mainly H2O2, and several LOPs, mainly 4-HNE (4-hydroxynonenal). Almost all H2O2 is kidnaped by erythrocytes (not reflected in this figure) if present. In nucleated cells, LOPs activates the NRF2 pathway, inducing the production of ARE (antioxidant response elements) and blocking the NFKB pathway. A small amount of H2O2 stimulates the NFKB pahtway, usually balanced with the NRF2 blocking action, producing a inmmunomodulation.
Several authors have published preclinical studies on the effects of medical ozone on living organisms, being able to demonstrate beneficial effects on the ability to modulate the redox balance, the cellular inflammation status, and the adaptation to ischemia/reperfusion processes (Barber et al., 1998; Peralta et al., 2000; Ajamieh et al., 2003, 2004, 2005).
From a clinical point of view, ozone therapy presents multiple medical-surgical applications, all of them related to the germicidal capacity of ozone, chronic ischemic and inflammation processes, and imbalance of the cellular redox status. Several manuals collect the experience and scientific work carried out to date by different research groups, mainly Italians, Germans, Russians, and Cubans (Bocci, 2002; Menéndez et al., 2008).
The forms of application of medical ozone are basically three: topical, infiltrative, and systemic (Baeza et al., 2015). Topical applications take advantage of the germicidal power of ozone and its positive effect on the healing processes; it is usually applied directly, with the use of zip-lock bags, or by using ozonated water or ozonated oils. Infiltrated ozone at concentrations between 4 and 30 μg/ml is useful for treating musculoskeletal diseases such as arthritis, tendonitis, myositis, fasciitis, neuritis, or myofascial pain. Systemic ozone therapy consists of the administration of the mixture of gasses mainly through two routes: the indirect intravenous way (also known as autohemotherapy) and the rectal insufflation. Indirect intravenous administration consists of extracting a determined blood quantity that, within a closed circuit, is put into contact with the gas, which will dissolve and react in a few seconds, and immediately reinfused. Certified (EU marked) medical devices should be used for this procedure. Rectal insufflation consists of administering a gas enema with a probe into the rectum, where it reacts with rectal mucus and generates peroxides. These are absorbed by the mucosa, reaching the hemorrhoidal plexus and the general venous blood circulation system like any other rectal treatment. The probes must be made of silicone or other ozone-resistant plastic (OzoneSolution, 2021).
Infiltrations With Medical Ozone (O2/O3)
Generalities
The use of O2/O3 infiltrations to treat musculoskeletal pathology is increasingly widespreading. Verga (1989) was the first to describe ozone intramuscular applications at the paravertebral level and trigger points in patients with chronic low back pain. Later, in the 90s, this procedure was also used to treat acute and chronic polyarthritis (hip, knee, sacroiliac joint, and interphalangeal), tendinitis, epicondylitis, carpal tunnel syndrome, and myofascial pain (Ajamieh et al., 2005).
Despite its frequent use, the level of evidence in many of the mentioned indications, but for the treatment of lumbar disk herniation and knee osteoarthritis, is low, possibly because it has been mainly used for years in private practice where randomized clinical trials are difficult to carry out. Carmona (2005) published in 2005 a systematic review on the efficacy of ozone therapy in rheumatic diseases, concluding that there were no quality clinical trials, that most of the works were published in low-impact journals, and that the methodology between the different studies is highly variable. However, this situation is changing, as more countries are using medical ozone in public centers and universities.
Therapeutic Properties and Mechanisms of Action of Injected Ozone
When we infiltrate the oxygen/ozone mixture, we are infiltrating a highly oxidizing gas, with a good tissue diffusion capacity. Apart from the general biochemical effect described in the Introduction section, several authors have described the anti-inflammatory, analgesic, and anti-edema properties of injected medical ozone, and propose that the oxidation of the algogenic receptors would inhibit the pain signal and it would activate the antinociceptive system (Re et al., 2010). This fact has been checked in one preclinical study from Fuccio et al. (2009) by inducing sciatic damage in mice, He confirmed the corticofrontal activation of genes of caspase 1, 8, and 12 (pro-inflammatory, pro-apoptotic, and responsible for allodynia) caused by the injury; this expression was normalized with a single peripheral injection of O2/O3 around the damaged area, which also reduced mechanical allodynia.
These properties would favor a muscle relaxant effect, as well as improved mobility of the treated area that can be observed clinically (Siemsen, 1995). This fact is very important in muscle recovery with O2/O3 injections. Balkanyi (1989) has described the utility of ozone therapy in the treatment of painful muscle hypertonia, highlighting the tremendous muscle relaxant effect that is produced.
Regarding the nucleus pulposus of the intervertebral disk, several authors have described that ROS will react with amino acids and carbohydrates of proteoglycans and collagen I and II that make up the matrix, giving a lead to a process of “mummification” which would shrink the disk, reducing the compression (Hawkins and Davies, 1996; Bocci et al., 2001; Leonardi et al., 2001). Iliakis and his group studied the histological changes of the nucleus pulposus matrix after treatment with an ozone intradiscal injection at a concentration of 27 μg/ml in rabbits and humans (resected disk specimens using microdiscectomy after the failure of the ozone treatment). Five weeks after the injection there were no signs of perilesional chondrocytic hyperplasia or inflammatory infiltrates typically observed in herniated disks biopsies; there was a fibrous tissue of less volume (“disk mummified”), which supposes a decrease in compression on the nerve root, a decrease in venous ecstasy, an improvement in local circulation, greater oxygenation and less pain, given the great sensitivity to hypoxia of nerve roots (Iliakis et al., 2001). Similar findings in pigs at different ozone concentrations were reported by Muto (2004).
Dosage
Regarding dosage, standardized protocols are lacking. Most authors relate the amount of the gas mixture to the extension of the injury or to the size of the joint cavity to be infiltrated. Generally, the amounts of gas range between 5 and 15 ml, and ozone concentrations range from 4 to 30 μg/ml. The number of infiltration sessions usually ranges from 3 to 10 (usually one or two per week) depending on the specific evolution of each case. About intradiscal injection, 2 ml for cervical and 5 for ml is the most used amount. If a patient does not respond to treatment after two or three interventions (once every 2 weeks) it is considered a failure. Torres et al. (2009) in a 2009 publication, after having used different concentrations with the same clinical protocol, observed more improvements when intradiscal O2/O3 is infiltrated at 50 μg/ml compared to lower concentrations (25 and 30 μg/ml). Nevertheless, we recommend not reaching 50 μg/ml due to the risk of iatrogenic injuries on the ring that have been detected experimentally in pigs (Muto, 2004).
This lack of standardization in the treatment protocols makes difficult to compare results when performing a systematic review, not allowing to get high quality conclusions or recommendations.
Ozone Therapy in Knee Pathology
One of the historic references was done in 1989 by Riva (1989), that registered 156 patients with knee joint pathology (post-traumatic arthritis, knee osteoathritis with mild deformity, and knee osteoathritis with severe deformity) obtaining good results that were especially positive when there were no severe bone deformities. The treatment consisted of intra-articular and periarticular infiltrations of 10 ml of medical ozone at a concentration of 20 μg/ml.
Later, In Cuba, a prospective study was carried out in 1997 to evaluate the efficacy and safety of medical ozone injections in 126 patients with knee osteoarthritis; usually, three or four injections were needed to obtain positive results, and only 14 patients received more than five sessions. 71.4% of the patients had a good result, in 10.3% the result was fair, and in 18.3% the result was bad. The main complication was pain during infiltration. It was highlighted the economic savings due to the low cost of the infiltrations and the lesser need for anti-inflammatory drugs (Escarpanter et al., 1997). Several authors have also published their experience in case series (Delgado and Quesada, 2005; Huanqui et al., 2006) and even proposed a treatment guide for based on their personal experience (Gheza and Bissolotti, 2003).
Moretti et al. (2004a) worked on the early knee osteoarthritis, comparing intraarticular injected O2/O3 with intraarticular hyaluronic acid, concluding that although there were no statistically significant differences in efficacy, ozone could be more indicated in the early stages of this disease, where inflammation predominates. In the same line, Giombini et al. (2016) published a randomized control trial comparing three kinds of injections: medical ozone, hyaluronic acid, and the combination. This last group showed the best outcomes and the hyaluronic acid group was more effective than ozone but without statistically significant differences. A systematic review and meta-analysis from Li et al. (2018) comparing medical ozone and hyaluronic acid had similar results, checking that hyaluronic acid was better than ozone but both improved the clinical status of the patients and had no significant side effects. A publication from Lopes de Jesus et al. (2017) demonstrated through a multicenter randomized, double-blind clinical trial the efficacy of intra-articular ozone injections versus placebo in knee osteoarthritis. In 2018 (Anzolin and Bertol, 2018; Costa et al., 2018; Raeissadat et al., 2018), 2019 (Arias-Vázquez et al., 2019; Noori-Zadeh et al., 2019) and 2020 (Sconza et al., 2020), six systematic reviews and meta-analyses were published in different journals supporting the use of ozone in knee osteoarthritis with a high level of evidence (GRADE 1+; Table 1).
These studies do not compare the results according to the radiological status of the knee, and we think this is basic fact, because hyaluronic acid is not indicated for moderate or severe knee osteoarthritis. Further studies in this line are needed to clarify the indications for medical ozone. Cost-efficacy studies are also needed as medical ozone is far cheaper than hyaluronic acid.
Other inflammatory knee pathologies have also been studied. Peritendinosus injected ozone has been used with success in refractory knee tendinopathies (Gjonovich et al., 2003). They improved 36 athletes with “jumper’s knee” who had not improved after conventional treatments.
Patellofemoral chondromalacia is a painful pathology whose treatment is mainly surgical, after which there is often aftermath. Manzi and Raimondi (2002) treated 60 patients with injected O2/O3 that had persistent pain after conventional surgical treatment, obtaining a higher and faster resolution of the pain in the treatment group compared to the control group.
Ozone Therapy in Shoulder Pathology
Gjonovich et al. (2002) published a prospective controlled study of patients suffering from subacromial tendinopathy treated with injected ozone versus mesotherapy; the ozone group showed superior clinical results. Ikonomidis et al. (2002) demonstrated in a double-blind clinical trial the greater efficacy of injected O2/O3 versus steroid injections and physiotherapy also in subacromial tendinopathy.
Oxygen-ozone therapy has also been used successfully in combination with shock waves, to treat calcifying tendinitis of the shoulder (Trenti and Gheza, 2002). Brina and Villani (2004) have published the utility of ultrasound-guided O2/O3 infiltrations in patients with non-surgical lesions of the rotator cuff. Medical ozone can increase the efficacy of other substances, as it was shown in paper of Moretti (2011) with hyaluronic acid and in paper of Gurger et al. (2021) with platelet-rich plasma (PRP); this last paper verifies the collaborative effect of ozone and PRP from a histological point of view.
Ozone Therapy in Spinal Pathology
Undoubtedly, the largest number of published works focuses on the use of ozone therapy for the treatment of herniated disks, both cervical and lumbar.
The treatment of cervical herniated disks is generally more conservative than that of the lumbar, perhaps due to the higher index of serious complications from your surgery (Wang et al., 2007). In this context, the interest in intradiscal or paravertebral medical ozone injections has special relevance, and the analgesic, anti-inflammatory, and muscle relaxant effects of the ozone therapy in cervical pathology have been described (Albertini, 2002; Villa, 2002).
In 2004, Moretti et al. (2004b), conducted a clinical trial comparing the efficacy of ozone therapy versus mesotherapy in patients with neck pain, upper limb paresthesias (uni or bilateral), peripheral vertigo, and headache. One hundred and fifty two patients had hernias, protrusions, or spondylosis, 76 of which were treated with medical ozone infiltrations in paravertebral muscles, the trapezius, and the elevators of the scapula; the other 76 patients were treated with anti-inflammatory drugs and mesotherapy. The differences were statistically significant in favor of the group treated with oxygen-ozone with 78% of optimal or good results, compared to 56.25% in the group of mesotherapy.
Regarding cervical intradiscal injections, a work published by Xiao et al. (2006) also supports their efficacy. Eighty-six patients with cervical spondylosis treated with CT-guided infiltrations were retrospectively assessed. Thirty-seven suffered from myelopathy, 30 had radiculopathy and 19 had sympathetic symptoms. The indication for treatment was cervicalgia with neurological symptoms (brachial irradiation patterns, loss of tenderness, tingling, numbness, muscle weakness, or deficiency of deep tendon reflexes) and all should be refractory to conservative therapies for at least 12 weeks. Patients with cervical spinal stenosis, ossification of the posterior longitudinal ligament were excluded. The treatment with ozone therapy was excellent, good, or poor in 78, 16, and 6% of the cases, respectively, as recorded with the modified MacNab Scale. These results coincide with those published by Alexandre et al. (2005) in the same year.
In lumbar pathology the number of published works is large. The good results, along with the safety of the technique and the dreaded complications of the surgery, have made more and more authors consider ozone therapy, either paravertebral or intradiscal, the first choice in case of failure of conservative treatment.
Andreula et al. (2003) added intradiscal and periganglionic O2/O3 to the infiltration with local anesthetics and steroids; in the 6 months follow-up, by blind evaluators, a statistically significant improvement was observed with the combination of both treatments. No side effect was detected. Buric et al. (2003) did a prospective follow-up over 18 months of 104 patients with lumbosciatic pain due to disk protrusions treated with intradiscal and intraforaminal O2/O3 injections, finding improvements in pain and functional capacity in most of them. Disk volume measurements were made with MRI and it was observed that, at 5 months, 22% of the protrusions had not changed in volume, 41% had reduced the size and 37% had disappeared. The results indicated that the technique was effective in the treatment of protrusions, although the efficacy was not higher than that of the microdiscectomy, according to the authors’ experience (Buric, 2005). Also regarding disk protrusions, Qing et al. (2005), in a sample of 602 patients and 1,078 operated disks, concluded the suitability treatment with ozone therapy as the first choice after failure more conservative techniques. When comparing ozone therapy with other minimally invasive techniques, these authors considered that it was an effective, safe, and minimally stressful technique for the patient and easy to perform.
Bonetti et al. (2005), in a randomized clinical trial, compared the efficacy of intraforaminal infiltration of O2/O3 with periradicular infiltration of steroids. Three hundred and six patients with low back pain and neuropathic leg pain with and without disk disease (spondylosis, spondylolisthesis, and facet joint degeneration) were recruited and randomly divided into two groups (166 and 140). The main measuring instrument was the modified MacNab scale. Patients were evaluated in the short (1 week), medium (3 months), and long term (6 months). In short term, there were no statistically significant differences between the two treatment modalities (p = 0.4077). In long term, the differences in favor of ozone treatments were statistically significant, but only in the group of patients with disk disease (p = 0.0021); also in long term, it could be seen that ozone therapy treatments had statistically lower failure rate (8.6%) than treatments with steroids (21.4%).
Muto et al. (2008) performed CT-guided injections to 2,900 patients with lumbosciatic pain due to herniated disks (including relapses). The gas was injected intradiscal, peri-ganglionic, and periradicular. After a month the patients were reviewed, repeating the session in those cases in which the improvement was partial. At 6 and 12 months, there were improvements of 75–80% with simple disk herniation, 70% with multiple hernias, and 55% with relapses.
Equally positive results are obtained by Castro et al. (2009), in a prospective observational study in which they treated 41 patients with simultaneous intradiscal, epidural, and periradicular infiltrations. Patients with a herniated disk and free fragment and/or major neurological deficit were excluded. The evolution was very positive (according to the VAS and the Laitinen test) from the first to the last of the post-basal records (at 30 days and 6 months, respectively), and the degree of satisfaction was rated as good by 85.4% of the sample.
To clarify the long term results of this technique, Torres et al. (2009) designed a study in patients with sciatica due to herniated disc by applying three consecutive sessions of O2/O3 infiltrations once a week; the first two with an epidural [adding bupivacaine (5 ml to 0.25%) and triamcinolone (4 mg)] and paravertebral ozone and the third one, only with intradiscal ozone. The evolution of 91 patients was recorded for 24 months. A very significant improvement was achieved in 95.6% of the patients at the first-month follow-up visit, 87.7% at the first-year visit, and persisted at the end of the follow-up in 84.1% of the sample. They got one case of discitis and 11 cases of temporary headache and four cases of temporary low back pain. They found a significant reduction of the size of the hernia in 79% of the patients at 24 months MRI.
Although most of the works published refer to intradiscal injections, paravertebral injections are safer, more simple, and the most used in clinical practice, although their efficacy was under discussion. In 2006, a randomized clinical trial was published (Zambello et al., 2006) comparing the efficacy of muscular paravertebral infiltration of O2/O3 with that of epidural steroids in patients refractory to conventional treatment (oral steroids and muscle relaxants). One hundred and seventy one patients were treated with epidural steroids and 180 underwent paravertebral infiltrations of medical ozone. At the 3 weeks follow-up, the improvement was statistically significant in favor of patients treated with ozone therapy (total or almost total remission of pain in 88.2%, compared to 59% in the steroids group), and at 6 months the evolution was excellent or good in 77.1% of patients treated with ozone therapy, compared to 47.3% of patients treated with steroids.
A double-blind randomized clinical trial was conducted (Paoloni et al., 2009) to better assess the efficacy of paravertebral ozone infiltrations in the treatment of acute low back pain due to herniated disk. Sixty patients were recruited and randomized into two groups; one was treated with real infiltrations and in the other group these were simulated. Follow-up was done 15, 30, 90, and 180 days after ending the treatment. Patients treated with true ozone injections significantly improved the pain and functional limitation (p < 0.05), requiring less analgesic medication.
In 2010, a meta-analysis was published (Steppan et al., 2010) on the efficacy and safety of ozone therapy for the treatment of herniated disks. Twelve studies were included with a total sample of 8,000 patients; the mean improvements recorded were similar to those reported for discectomy: 3.9 points out of 10 on the visual analog pain scale, 25.7 points in functional capacity according to the Oswestry Disability Index and a 79.7% improvement in the records of the modified MacNab scale. The percentage of complications was 0.064%, so the treatment was considered safe and effective. Two years later, Magalhaes et al. (2012) published a systematic review and meta-analysis compiling eight observational studies and four randomized clinical trials. They concluded that the intradiscal injection to treat lumbar disk herniation has a recommendation level of 1C and that the paravertebral treatment has a recommendation level 1B according to the criteria of the US Preventive Services Task Force; this means that the recommendation is strong (maximum level), although with certain reservations for intradiscal injection due to the diversity of existing protocols.
About 80% of the population in Western countries will experience at least one episode of low back pain in your lifetime, and 55% of these will have an associated radicular pain (Long, 1991). Failed back surgery syndrome ranges between 15% and 20%, which leads to propose more conservative and less invasive treatments, such as ozone therapy, whose effectiveness seems to oscillate between 65 and 80% suggesting that a small change in disk volume can produce a large clinical change (Gangi et al., 1998). Complications of open surgery must also be taken into account, such as fibrosis, epidural and perineural tears, nerve adhesions, limitations of biomechanics due to fibrosis, and muscle paravertebral spasms and associated myofascial syndromes (Manchikanti et al., 2007). In this context, infiltrations with O2/O3, both at the paravertebral level and trigger points of related musculature and percutaneous intradiscal injection with ozone, are techniques on the rise due to their efficacy, ease of execution, low cost, and very few important side effects.
Andreula et al. (2003), when comparing ozone intradiscal injection with enzymatic nucleolysis, conclude that, with similar clinical results, treatment with ozone therapy would be the first choice due to its advantages like the ones that follow:
•There is no possibility of allergic reactions or anaphylactic
•Possibility of repeating the treatment as many times as it is considered
•Theoretical lower risk of infections, due to the germicides properties of ozone
•Possibility of using a thinner needle due to ozone fluidity and, therefore, a so much less traumatic injection
•Less post-infiltration discomfort (2, 3 days vs. 1 or 2 weeks).
To these advantages would be added those described over corticosteroids due to the absence of ozone adverse effects. In this regard, Fernández et al. (1998), in their review on the use of corticosteroids draw attention to the following points:
•Infectious arthritis
•Progressive joint deterioration
•Soft-tissue atrophy and hypopigmentation
•Tendon rupture
•Reactive synovitis due to glucocorticoid microcrystals
•Systemic adverse effects.
Some recent publications remark that the ozone administration does not close the path to surgery in case of failure (Bocci et al., 2015; Muto et al., 2016).
Finally, it is worth mentioning that the efficacy of ozone therapy in the treatment of failed back surgery syndrome, highly prevalent among spine-operated patients, and usually worsens with new surgeries. In these patients, we observe fibrosis due to epidural and perineural scars, paravertebral spasms, and neural adhesions, whose chronic inflammatory stimulus would lead to neuroplastic phenomena with central and peripheral sensitization. Theoretically, the fibrinolytic, anti-inflammatory and antioxidant properties of the infiltrated O2/O3 would make it ideal for the treatment of these processes. The team from the National Medical Center 20 de Noviembre, in Mexico City, has published two papers treating 30 patients in each work. On both studies applied a first epidural injection together paravertebral infiltration followed by three weekly sessions of paravertebral infiltrations; doses of 20 ml at 30 μg/ml in the first paper and the same amount at 50 μg/ml in the second one, but the treatments could not improve patients’ pain (Grijalva et al., 2012; Hernández et al., 2012). A promising alternative would be the combination of repeated paravertebral injections combined with epidural ones. Padilla del Rey et al. (2015) reported very significant improvement (VAS of 10 a 3) in a patient with refractory post-laminectomy pain who received three epidural infiltrations with ozone (10 ml at 20 μg/ml concentration) in three consecutive weeks and six paravertebral infiltrations, twice a week at the same time (10 ml at 10–30 μg/ml progressive concentration). Anyway, given the scale of the problem, more studies are needed.
Infiltrative Ozone Therapy in Rheumatoid Arthritis
A preclinical study carried out in Nanfang Hospital compared the effects of medical ozone infiltrations at different concentrations compared to oxygen; the authors showed that intra-articular ozone injected at a concentration of 40 μg/ml is capable of inhibiting synovitis in rats with rheumatoid arthritis (Chen et al., 2013). Some doctors use ozone therapy empirically in patients with rheumatic diseases using joint infiltrations for years, supposedly with very positive results, but there are no major works published in this regard.
As mentioned, ozone therapy would be indicated as an adjuvant treatment of diseases related to disturbance of cellular redox balance or tissue oxygenation. From this point of view, systemic ozone therapy would help patients with pain chronic, as recent preclinical studies have demonstrated the role of ROS in hyperalgesia, via activation of the N-methyl-D-aspartate (NMDA) receptors. Gao et al. (2007), in a preclinical model of pain, both neuropathic and inflammatory, could demonstrate that ROS were increased at the dorsal horn in these patients, and that systemic administration of a neutralizing agent of ROS reduced the hyperalgesia by blocking phosphorylation from NMDAs. Later, the same research group (inducing hyperalgesia by capsaicin in rats) was able to demonstrate the role of the superoxide anion as responsible for abnormal pain signal processing in the dorsal horn, suggesting the therapeutic role of mitochondrial SOD-2 in these types of pain (Schwartz et al., 2009).
But certainly, the levels of scientific evidence in the treatment with systemic ozone therapy for chronic pain are practically non-existent. In this regard, a study by Clavo et al. (2013), on chronic headache refractory to triptans, found that systemic ozone improved pain and frequency of crises. Also, Fernández et al. (2016) published a work in which the use of systemic ozone therapy improved efficacy and decreased the side effects of methotrexate in patients with rheumatoid arthritis. Theoretically, the beneficial effect on immunosuppressed patients would make it useful, both in the treatment of herpes zoster infection and postherpetic neuralgia (Hu et al., 2018). In this field, several experts have tried ozone treatments for years, apparently with positive results. Ozone therapy is generally used as an adjunct to conventional treatments, either systemic or local (infiltrations or applications of oils and ozonated water; Mattassi et al., 1985; Delgado et al., 1989; Konrad, 2001). These studies have a low evidence level but are useful to encourage the development of better-designed works.
Fibromyalgia seems to be a “stress disease” in which underlies an alteration of the cellular redox balance, consequence of an increase in the production of free radicals, a deficiency of organic antioxidant capacity, or both simultaneously. Biochemical findings support this fact and systemic ozone therapy has been proposed (Borrelli and Bocci, 2002; Hidalgo, 2012). Hidalgo et al. (2005) treated 21 patients with fibromyalgia refractory to a multidisciplinary treatment with 10 sessions of autohemotherapy, finding very good tolerability and improvement in pain and fatigue, as well as a significant decrease in the use of pain medication. This same research group (Hidalgo-Tallón et al., 2013) treated 36 patients with fibromyalgia with one daily dose of rectal ozone (200 ml of gas at 40 μg/ml) during 24 sessions, reporting significant improvements in the Fibromyalgia Impact Questionnaire, the state of mind, and the physical component of the quality of life using SF-12 scale. The treatment was very well tolerated, with transient meteorism as the most relevant adverse effect.
Systemic ozone has also been tested together with infiltrations in patients with rheumatoid arthritis. A Calunga et al. (2007) research group, published a study about lumbar disk herniation comparing paravertebral infiltrations isolated or combined with rectal ozone and checked that the combination improved all clinical parameters. In 2010, they compared (Méndez-Pérez et al., 2010) isolated O2/O3 intra-articular infiltrations (3 ml at 10 μg/ml) with the infiltrations plus rectal ozone in patients with rheumatoid arthritis of the temporomandibular joint; improvements, both in pain and in function and state of the joint capsule were statistically significant in favor of the combination therapy. In this regard, systemic ozone therapy seems to decrease in these patients interleukin 1 beta levels, directly related to disease activity, while intraarticular ozone injections would decrease intraarticular interleukin 8 levels, justifying lower granulocyte count and clinical improvement (Eastgate et al., 1988; Menéndez et al., 1989; Fahmy, 1993, 1995).
Safety and Contraindications of Ozone Therapy
All authors agree on the high safety of treatments with ozone therapy, especially modern medical ozone generators with great precision.
Jacobs (1982) published that the incidence of effects adverse effects of systemic ozone therapy was only 0.0007%, mainly nausea, headache, and fatigue. In Cuba, with 25 years of experience, having at least one ozone therapy unit per province of the country, only slight adverse effects have been recorded (Bocci, 2002).
The experience of Italian experts is similar, although Dr. Bocci (Ajamieh et al., 2005) describes at least six deaths from gas applications in a direct intravenous way, a practice not recommended by scientific associations (Baeza et al., 2015).
Eventually, the most serious common adverse effect would be a vagal reaction, generally associated with pain during infiltration. It is necessary to note that the injection must be done slowly, especially if a large gas volume at a high concentration is used (Zambello et al., 2004).
An absolute contraindication is severe glucose-6 deficiency phosphate dehydrogenase (favism), as this enzyme is necessary for supply hydrogen ions to the glutathione system, responsible for buffering the oxidation that lipoperoxides will produce in red blood cells (Viebahn, 2007).
As relative contraindications to systemic ozone therapy would be uncontrolled hyperthyroidism, thrombocytopenia, severe cardiovascular instability, and seizure states. It is also not advisable to use systemic ozone therapy in pregnant patients (Bocci, 2002) as it has not been deeply tested. Infiltrations should be avoided following the general criteria described in the literature (Sánchez et al., 2006).
Undoubtedly, ozone therapy should be practiced by a well-trained doctor and, in patients with a poor general condition, a diagnosis of the pro-oxidant/antioxidant status of the patient would be advisable.
Conclusion
For knee osteoarthritis and lumbar disk herniation, evidence on safety and efficacy from systematic reviews and meta-analysis, according the quality of the evidences proposed by the Scottish Intercollegiate Guidelines Network (SIGN), including GRADE criteria, are high (1+ and 2+ studies) and allow a recommendation level B, the same observed in most of the techniques used presently in pain units (SIGN, 2019).
However, for the rest of potential indications, the evidence level is low and ozone must be used only when other conventional treatments have failed or in a compassionate way.
Lack of standardization in treatment protocols is the Achilles’ heel of this technique, probably because of his great tolerablity that encourage doctors to explore different dosages without comparing efficacy between them. This is the main criticism in systematic reviews’ conclusions.
More RCT are needed to increase our knowledge on the indications of medical ozone, but safety profile is good enough so as to develop them. Fortunately, research interest on ozone therapy is growing, as we can check by simply doing a basic research in PubMed and watching the evolution of the number of publications in the past 20 years.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Ajamieh, H. H., Berlanga, J., Merino, N., Sánchez, G. M., Carmona, A. M., Cepero, S. M., et al. (2005). Role of protein synthesis in the protection conferred by ozone – oxidative – preconditioning in hepatic ischemia/reperfusion. Transpl. Int. 18, 604–612. doi: 10.1111/j.1432-2277.2005.00101.x
Ajamieh, H. H., Menéndez, S., Martínez-Sánchez, G., Candelario-Jalil, E., Re, L., Giuliani, A., et al. (2004). Effects of ozone oxidative preconditioning on nitric oxide generation and cellular redox balance in a rat model of hepatic ischemia – reperfusion. Liver Int. 24, 55–62. doi: 10.1111/j.1478-3231.2004.00885.x
Ajamieh, H. H., Menéndez, S., Merino, N., Martinez-Sanchez, G., Re, L., and León, O. S. (2003). Ischemic and ozone oxidative preconditioning in the protection against hepatic ischemic-reperfusion injury. Ozone Sci. Eng. 25, 241–250. doi: 10.1080/01919510390481568
Alexandre, A., Coro, L., Azuelos, A., Buric, J., Salgado, H., Murga, M., et al. (2005). “Intradiscal injection of oxygen-ozone gas mixture for the treatment of cervical disc herniations,” in Advanced Peripheral Nerve Surgery and Minimal Invasive Spinal Surgery. ed. A. Alexandre. Vienna: Springer.
Andreula, C. F., Simonetti, L., De Santis, F., Agati, R., Ricci, R., and Leonardi, M. (2003). Minimally invasive oxygen-ozone therapy for lumbar disk herniation. Am. J. Neuroradiol. 24, 996–1000.
Anzolin, A. P., and Bertol, C. D. (2018). Ozonioterapia como terapêutica integrativa no tratamento da osteoartrose: uma revisão sistemática. Br. J. Pain 1, 171–175. doi: 10.5935/2595-0118.20180033
Arias-Vázquez, P. I., Tovilla-Zárate, C. A., Bermudez-Ocaña, D. Y., Legorreta-Ramírez, B. G., and López-Narváez, M. L. (2019). Eficacia de las infiltraciones con ozono en el tratamiento de la osteoartritis de rodilla vs. otros tratamientos intervencionistas: revisión sistemática de ensayos clínicos. Rehabilitación. 53, 43–55. doi: 10.1016/j.rh.2018.11.001
Babaei-Ghazani, A., Karimi, N., Forogh, B., Madani, S. P., Ebadi, S., Fadavi, H. R., et al. (2019). Comparison of ultrasound-guided local ozone (O2-O3) injection vs corticosteroid injection in the treatment of chronic plantar fasciitis: a randomized clinical trial. Pain Med. 20, 314–322. doi: 10.1093/pm/pny066
Balan, C., Schiopu, M., Balasa, D., and Balan, C. (2017). Ozone therapy – a rare and avoidable source of infectious pathology of the spine. Rom Neurosurg. 31:46. doi: 10.1515/romneu-2017-0046
Balkanyi, A. (1989). “The interaction between ozone therapy and oxygen radicals and their importance in practice.” in Proceedings of the Ninth Ozone World Congress; June 3–9, 1989; New York; 22–27.
Barber, E., Menéndez, S., Barber, M. O., Merino, N., and Calunga, J. L. (1998). Functional and morphological renal study in kidneys of rats pretreated with ozone and subjected to warm ischemia. CENIC Biol. Sci. 29, 178–181.
Bocci, V., Borrelli, E., Zanardi, I., and Travagli, V. (2015). The usefulness of ozone treatment in spinal pain. Drug Des. Devel. Ther. 9:2677. doi: 10.2147/DDDT.S74518
Bonetti, M. (2003). CT-guided oxygen-ozone infiltration into isthmic lysis points in the management of 1st negree spondylolisthesis and spondylolysis. Riv. Ital. Ossigeno-Ozone Ther. 2, 31–38.
Bonetti, M., Cotticelli, B., Richelmi, P., and Valdenassi, L. (2002). Rofecoxib e O2-O3 therapy vs O2-O3 therapy in the spondyloarthrosis treatment. Riv. Ital. Ossigeno-Ozone Ther. 1, 171–178.
Bonetti, M., Fontana, A., Cotticelli, B., Dalla Volta, G., Guindani, M., and Leonardi, M. (2005). Intraforaminal O2-O3 versus periradicular steroidal infiltrations in lower back pain: randomized controlled study. Am. J. Neuroradiol. 26, 996–1000.
Bonetti, M., Moretti, M., Guarino, G., and Bragaglio, G. (2011). Rhizoarthrosis: our experience with oxygen-ozone treatment. Riv. Ital. Ossigeno-Ozone Ther 10, 63–63.
Borrelli, E., and Bocci, V. (2002). A novel therapeutic option for chronic fatigue syndrome and fibromyalgia. Riv. Ital. Ossigeno-Ozone Ther. 1, 149–153.
Brina, L., and Villani, P. C. (2004). Treatment of rotator cuff lesions with echo-guided infiltration of an oxygen-ozone mixture. Riv. Ital. Ossigeno-Ozone Ther. 3, 139–147.
Buric, J. (2005). Ozone chemyonucleolysis vs microdiscectoy. Prospective controlled study with 18 months follow-up. Riv. Ital. Ossigeno-Ozone Ther. 4, 49–54.
Calunga, J. L., Ramos, T. L., Castillo, P., Menéndez, S., Carballo, A., and Céspedes, J. (2007). Ozonoterapia combinada en el tratamiento del paciente portador de hernia discal lumbar: estudio preliminar. Rev Cubana Invest Bioméd [Internet]. 2007 Mar [cited 2021 Nov 30]; 26. Available in: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-03002007000100003&lng=esn
Cano, P. A., Vela, T., Cano, C., García, G., Vera, J. C., and Andrés-García, J. A. (2016). Cervical spondylodiscitis after oxygen–ozone therapy for treatment of a cervical disc herniation: a case report and review of the literature. HSSJ. 12, 278–283. doi: 10.1007/s11420-016-9500-1
Chen, H., Yu, B., Lu, C., and Lin, Q. (2013). The effect of intra-articular injection of different concentrations of ozone on the level of TNF-α, TNF-R1, and TNF-R2 in rats with rheumatoid arthritis. Rheumatol. Int. 33, 1223–1227. doi: 10.1007/s00296-012-2529-7
Corea, F., Amici, S., Murgia, N., and Tambasco, N. (2004). A case of vertebrobasilar stroke during oxygen-ozone therapy. J. Stroke Cerebrovasc. Dis. 13, 259–261. doi: 10.1016/j.jstrokecerebrovasdis.2004.08.004
Escarpanter, J. C., Valdés, O., Sánchez, R., López, Y., and López, C. (1997). Therapeutic results in osteoarthritis of the knee with ozone infiltrations. Rev. Cuba. Investig. Biomed. 16, 124–132.
Fahmy, Z. (1993). “Immunological effect of ozone (O2-O3) in rheumatic diseases.” in Proceedings of the Eleventh Ozone World Congress, Ozone in Medicine. (Stamford, Conn.: International Ozone Association); August 29 - September 3, 1993; San Francisco, CA, USA.
Fahmy, Z. (1995). “Correlation of plasma interleukin 1 levels with disease activity in rheumatoid arthritis with and without Ozone.” in Proceedings of the 12th Ozone World Congress (Stamford, Conn.: International Ozone Association); May 15-18, 1995; Lille, France.
Fernández, O. S. L., Viebahn-Haensler, R., Cabreja, G. L., Espinosa, I. S., Matos, Y. H., Roche, L. D., et al. (2016). Medical ozone increases methotrexate clinical response and improves cellular redox balance in patients with rheumatoid arthritis. Eur. J. Pharmacol. 789, 313–318. doi: 10.1016/j.ejphar.2016.07.031
Fernández-Cuadros, M. E., Pérez-Moro, O., Albaladejo-Florin, M. J., and Álava-Rabasa, S. (2020). El ozono intrarticular modula la inflamación, mejora el dolor, la rigidez, la función y tiene un efecto anabólico sobre la artrosis de rodilla: estudio cuasiexperimental prospectivo tipo antes-después, 115 pacientes. Rev Soc Esp Dolor. 27, 78–88. doi: 10.20986/resed.2020.3775/2019
Fort, N. M., Aichmair, A., Miller, A. O., and Girardi, P. (2014). L5–S1 Achromobacter xylosoxidans infection. Spine 39, E413–E416. doi: 10.1097/BRS.0000000000000195
Fuccio, C., Luongo, C., Capodanno, P., Giordano, C., Scafuro, M. A., Siniscalco, D., et al. (2009). A single subcutaneous injection of ozone prevents allodynia and decreases the over-expression of pro-inflammatory caspases in the orbito-frontal cortex of neuropathic mice. Eur. J. Pharmacol. 603, 42–49. doi: 10.1016/j.ejphar.2008.11.060
Gaffuri, M., Garaffo, R., and Gheza, G. (2003). Oxygen-ozone therapy for lateral humeral epicondylitis: preliminary findings. Riv. It Ossigeno-Ozone Ther. 2, 169–172.
Gangi, A., Dietemann, J. L., Mortazavi, R., Pfleger, D., Kauff, C., and Roy, C. (1998). CT-guided interventional procedures for pain management in the lumbosacral spine. Radiographics 18, 621–633. doi: 10.1148/radiographics.18.3.9599387
Gao, X., Kim, H. K., Chung, J. M., and Chung, K. (2007). Reactive oxygen species (ROS) are involved in enhancement of NMDA-receptor phosphorylation in animal models of pain. Pain 131, 262–271. doi: 10.1016/j.pain.2007.01.011
Gazzeri, R., Galarza, M., Neroni, M., Esposito, S., and Alfieri, A. (2007). Fulminating septicemia secondary to oxygen-ozone therapy for lumbar disc herniation. Case Rep. 32, E121–E123. doi: 10.1097/01.brs.0000254125.85406.6e
Gheza, G. (2002). Metatarsalgia trattata with O2-O3 in peace with fibrosis post-chirurgical scarring of Morton’s neuroma asportazione. Riv. Ital. Ossigeno-Ozone Ther. 1, 109–111.
Gheza, G., Ipprio, L., and Bissolotti, L. (2002). Oxygen-ozone therapy in a diabetic patient with De Quervain’s tenosynovitis associated with joint arthrosis. Riv. Ital. Ossigeno-Ozone Ther. 1, 189–192.
Ginanneschi, F., Cervelli, C., Milani, P., and Rossi, A. (2006). Ventral and dorsal root injury after oxygen-ozone therapy for lumbar disk herniation. Surg. Neurol. 66, 619–620. doi: 10.1016/j.surneu.2006.01.025
Giombini, A., Menotti, F., Di Cesare, A., Giovannangeli, F., Rizzo, M., Moffa, S., et al. (2016). Comparison between intrarticular injection of hyaluronic acid, oxygen ozone, and the combination of both in the treatment of knee osteoarthrosis. J. Biol. Regul. Homeost. Agents 30, 621–625.
Gjonovich, A., Girotto, L., Sattin, G. F., Girotto, T., and Preciso, G. (2002). Oxygen-ozone therapy in shoulder pain. Riv. Ital. Ossigeno-Ozone Ther. 1, 37–40.
Gjonovich, A., Marchetto, R., Montemarà, E., and Girotto, T. (2003). Refractory tendinopathies of the knee: use of oxygen-ozone therapy. Riv. Ital. Ossigeno-Ozone Ther. 2, 187–192.
Grijalva, Y. M., Hernández, J. R., Tenopala, S., Canseco, C. P., and Torres, J. C. (2012). Application efficiency of epidural and paravertebral ozone at a concentration of 50 μg/ml in patients with chronic pain secondary to postlaminectomy syndrome. Rev. Soc. Esp Dolor. 19, 66–71.
Gurger, M., Once, G., Yilmaz, E., Demir, S., Calik, I., Say, Y., et al. (2021). The effect of the platelet-rich plasma and ozone therapy on tendon-to-bone healing in the rabbit rotator cuff repair model. J. Orthop. Surg. Res. 16:202. doi: 10.1186/s13018-021-02320-w
Hawkins, C. L., and Davies, M. J. (1996). Direct detection and identification of radicals generated during the hydroxyl radical-induced degradation of hyaluronic acid and related materials. Free Radic. Biol. Med. 21, 275–290. doi: 10.1016/0891-5849(96)00042-1
He, R., Huang, Q., Yan, X., Liu, Y., Yang, J., and Chen, X. (2019). A case of paradoxical embolism causing anterior spinal cord syndrome and acute myocardial infarction following the Intradiscal oxygen-ozone therapy. Front. Neurol. 10:137. doi: 10.3389/fneur.2019.00137
Hernández, B. D., Hernández, J. R., Tenopala, S., Canseco, C. P., and Torres, J. C. (2012). Application efficiency epidural and paravertebral ozone at a concentration of 30 μg/ml for the management of chronic pain in patients with failed surgery syndrome back. Rev. Soc. Esp Dolor. 19, 3–10.
Hidalgo, F. J., Calandre, E., Rico, F., Delgado, A., Entrena, J. M., and Menéndez, S.. (2005). “Interest of systemic ozone in the treatment of highly refractory fibromyalgia.” in IV Jornadas Nacionales de Oxígeno-ozonoterapia médica. Noviembre 4-5, 2005; Sevilla (Spain).
Hidalgo-Tallón, F. J., Menéndez-Cepero, S., Vilchez, J. S., Rodríguez-López, C. M., and Calandre, E. P. (2013). Ozone therapy as add-on treatment in fibromyalgia management by rectal insufflation: an open-label pilot study. J. Altern. Complement. Med. 19, 238–242. doi: 10.1089/acm.2011.0739
Hu, B., Zheng, J., Liu, Q., Yang, Y., and Zhang, Y. (2018). The effect and safety of ozone autohemotherapy combined with pharmacological therapy in postherpetic neuralgia. J. Pain Res. 11, 1637–1643. doi: 10.2147/JPR.S154154
Huanqui, C., Cruz, M., Miranda, A., Poblete, P., and Mamani, R. (2006). Effectiveness and safety of intra-articular ozone in knee osteoarthritis refractory to treatment. UCSM 12, 21–26.
Hüseyin, T., Uğur, Ö., Hasan, K., and Nurettin, L. (2017). Severe headache following ozone therapy: Pneumocephalus. Agri 29, 132–136. doi: 10.5505/agri.2016.36024
Ikonomides, S. T., Iliakis, E. M., Eleftheriadou, A., Bratanis, D., and Thomaidis, R. (2003). Conservative treatment of acute or chronic tendonitis with oxygen-ozone mixture. Riv. Ital. Ossigeno-Ozone Ther. 2, 67–71.
Ikonomidis, S. T., Iliakis, E. M., and Charalambus, L. (2002). Nonoperative treatment of shoulder impingement syndrome with topical injections of medical oxygen-ozone mixture. A double blind clinical trial. Riv. Ital. Ossigeno-Ozone Ther. 1, 41–44.
Iliakis, E., Valadakis, V., Vynios, D. H., Tsiganos, C. P., and Agapitos, E. (2001). Rationalization of the activity of medical ozone on intervertebral disc a histological and biochemical study. Riv. Neuroradiol. 14, 23–30. doi: 10.1177/19714009010140S105
Konrad, H. (2001). “Ozone therapy for postherpetic neuralgia. A retrospective study of 55 cases.” in Proceedings of the 15th Ozone World congress, Medical Therapy Conference (Stamford, Conn.: International Ozone Association). September 11-15, 2011; London, UK.
Leonardi, M., Simonetti, L., and Barbara, C. (2001). Effetti dell’ozono sul nucleo polposo: reperti anatomo-pathologici its an operative case. Riv. Neuroradiol. 14, 57–59. doi: 10.1177/19714009010140S113
Li, Q., Qi, X., and Zhang, Z. (2018). Intra-articular oxygen-ozone versus hyaluronic acid in knee osteoarthritis: A meta-analysis of randomized controlled trials. Int. J. Surg. 58, 3–10. doi: 10.1016/j.ijsu.2018.08.007
Lo Giudice, G., Valdi, F., Maurizio, G., Prosdocimo, G., and de Belvis, V. (2004). Acute bilateral vitreo-retinal hemorrhages following oxygen-ozone therapy for lumbar disk herniation. Am. J. Ophth. 138, 175–177. doi: 10.1016/j.ajo.2004.02.059
Lopes de Jesus, C. C., Dos Santos, F. C., de Jesus, L. M. O. B., Monteiro, I., Sant’Ana, M. S. S. C., and Trevisani, V. F. M. (2017). Comparison between intra-articular ozone and placebo in the treatment of knee osteoarthritis: a randomized, double-blinded, placebo-controlled study. PLoS One 12:e0179185. doi: 10.1371/journal.pone.0179185
Magalhaes, F. N., Dotta, L., Sasse, A., Teixeira, M. J., and Fonoff, E. T. (2012). Ozone therapy as a treatment for low back pain secondary to herniated disc: a systematic review and meta-analysis of randomized controlled trials. Pain Physician 15, E115–E129.
Manchikanti, L., Singh, V., Cash, K. A., Pampati, V., and Datta, S. (2007). Preliminary results of a randomized, equivalence trial of fluoroscopic caudal epidural injections in managing chronic low back pain: part 3 – post surgery syndrome. Pain Physician 11, 817–831.
Marchetti, D., and La Monaca, G. (2000). An unexpected death during oxygen-ozone therapy. Am. J. Forensic Med. Pathol. 21, 144–147. doi: 10.1097/00000433-200006000-00010
Mattassi, R., Bassi, P., D’Angelo, F., Franchina, A., and Sbrascini, S. (1985). “Ozone as therapy in herpes simplex and herpes zoster diseases,” in Medical Applications of Ozone. ed. J. LaRous (Norwalk: International Ozone Association), 134–137.
Méndez-Pérez, I., Cerro-Montesino, A. D., Cámbara-Peña, R., Martínez-Godíne, J., and Menéndez-Cepero, S. (2010). Systemic and intra-ozone therapy joint in arthritis of the temporomandibular joint from arthritis rheumatoid. CENIC Biol. Sci. 41, 169–172.
Menéndez, P., García, A., and Peláez, R. (2014). Absceso paravertebral e intraabdominal secundario a ozonoterapia por lumbalgia. Rev. Esp. Cir. Ortop. Traumatol. 58, 125–127. doi: 10.1016/j.recot.2013.06.003
Menéndez, S. A., González, R., Ledea, O. E., Hernández, F. A., León, O. S., and Díaz, M. F. (2008). Ozone Basic Aspects and Clinical Applications. Havana: CENIC.
Moretti, M. (2011). Effect of treatment with O2-O3 and hyaluronic acid in partial tear of the supraspinatus tendon. Riv. Ital. Ossigeno-Ozone Ther. 10:37.
Moretti, B., Lanzisera, R., Morese, A., Moretti, L., Patella, S., Patella, V., et al. (2004a). O2-O3 vs chondroprotectors in the treatment of osteoarthritis of the knee. Riv. Ital. Ossigeno-Ozone Ther. 3, 65–72.
Moretti, B., Lanzisera, R., Pesce, V., Moretti, L., Patella, S., and Patella, V. S. C. (2004b). O2-O3 vs. anti-inflammatory drugs in the treatment of neck pain. Riv. Ital. Ossigeno-Ozone Ther. 3, 131–137.
Mustafa, Ç., Yunus, C., and Şakir, B. (2015). Myocardial infarction after ozone therapy: is ozone therapy Dr. Jekyll or Mr. Hyde? Cardiology 132, 101–104. doi: 10.1159/000431078
Muto, M. (2004). Intradiscal and intramuscular injection of oxygen – ozone: pathological evaluation. Work in Progress. Riv. Ital. Ossigeno-Ozone Ther. 3, 7–13.
Muto, M., Giurazza, F., Silva, R. P., and Guarnieri, G. (2016). Rational approach, technique and selection criteria treating lumbar disk herniations by oxygen–ozone therapy. Interv. Neuroradiol. 22, 736–740. doi: 10.1177/1591019916659266
Noori-Zadeh, A., Bakhtiyari, S., Khooz, R., Haghani, K., and Darabi, S. (2019). Intra-articular ozone therapy efficiently attenuates pain in knee osteoarthritic subjects: a systematic review and meta-analysis. Complement. Ther. Med. 42, 240–247. doi: 10.1016/j.ctim.2018.11.023
Padilla del Rey, M. L., García Fernández, M. R., García Sánchez, F., Rastrollo Peña, D., Díaz-Alejo Marchante, C., and Gonzálvez Ortega, J. J., et al. (2015). “Ozone therapy in failed back surgery syndrome.” in 21st Annual Meeting ESRA. September 30 - October 2, 2015; Mallorca, Spain.
Palanca-Sánchez, I., Puig-Riera de Conías, M. M., Elola-Somoza, J., Bernal-Sobrino, J. L., and Paniagua Caparrós, J. L. (2011). Grupo de Expertos. Unidad de tratamiento de dolor: estándares y recomendaciones. Madrid: Ministerio de Sanidad, Política Social e Igualdad. Available at: https://www.mscbs.gob.es/organizacion/sns/planCalidadSNS/docs/EERR/Unidad_de_tratamiento_del_dolor.pdf (Accessed November 30, 2021).
Paoloni, M., Di Sante, L., Cacchio, A., Apuzzo, D., Marotta, S., Razzano, M., et al. (2009). Intramuscular oxygen-ozone therapy in the treatment of acute back pain with lumbar disc herniation: a multicenter, randomized, double-blind, clinical trial of active and simulated lumbar paravertebral injection. Spine 34, 1337–1344. doi: 10.1097/BRS.0b013e3181a3c18d
Peralta, C., Xaus, C., Bartrons, R., Leon, O. S., Gelpí, E., and Roselló-Catafau, J. (2000). Effect of ozone treatment on reactive oxygen species and adenosine production during hepatic ischemia-reperfusion. Free Radic. Res. 33, 595–605. doi: 10.1080/10715760000301121
Pressman, S. (2021). The story of ozone - 6th edition [Internet]. Santa Barbara Ca: Ozone Therapies Group; 2019 Oct [cited 2021 Nov 30]. Available from: https://www.ozonetherapiesgroup.com/ozone-research/2019/10/28/the-story-of-ozone-6th-edition
Raeissadat, S. A., Tabibian, E., Rayegani, S. M., Rahimi-Dehgolan, S., and Babaei-Ghazani, A. (2018). An investigation into the efficacy of intra-articular ozone (O2-O3) injection in patients with knee osteoarthritis: a systematic review and meta-analysis. J. Pain Res. 11, 2537–2550. doi: 10.2147/JPR.S175441
Salvatore, A., Valente, C., De Benedetti, G., and Caramello, G. (2016). Transient cortical blindness after intradiscal oxygen–ozone therapy. Indian J. Ophthalmol. 64:944. doi: 10.4103/0301-4738.198858
Sánchez, I., Ferrero, A., Aguilar, J. J., Conejero, J. A., Flórez, M. T., Arrebola, A., et al. (2006). SERMEF Manual of Rehabilitation and Physical Medicine. Madrid: Panamerican Medical.
Schwartz, E. S., Kim, H. Y., Wang, J., Lee, I., Klann, E., Chung, J. M., et al. (2009). Persistent pain is dependent on spinal mitochondrial antioxidant levels. J. Neurosci. 29, 159–168. doi: 10.1523/JNEUROSCI.3792-08.2009
Sconza, C., Respizzi, S., Virelli, L., Vandenbulcke, F., Iacono, F., Kon, E., et al. (2020). Oxygen-ozone therapy for the treatment of knee osteoarthritis: a systematic review of randomized controlled trials. Arthroscopy 36, 277–286. doi: 10.1016/j.arthro.2019.05.043
Seyman, D., Sepin, N., Inan, D., Ongu, G., and Ogunc, D. (2012). Pseudomonas aeruginosa septic arthritis of knee after intra-articular ozone injection. New Microbiol. 35, 345–348.
Siemsen, C. H. (1995). Ozon-Anwendung bei akuten und chronischen Gelenkerkrankungen. Ozon-Handbuch. Grundlagen. Prävention. Therapie. Landsberg: Ecomed.
Steppan, J., Meaders, T., Muto, M., and Murphy, K. J. (2010). A metaanalysis of the effectiveness and safety of ozone treatments for herniated lumbar discs. J. Vasc. Interv. Radiol. 21, 534–548. doi: 10.1016/j.jvir.2009.12.393
Torres, L. M., Terrero, M. J., Vidal, M., Aragón, F., and Martínez, J. (2009). Discolysis with intradiscal ozone in the treatment of sciatica due to herniated discs. Follow-up of 100 patients in 24 months. Rev. Soc. Esp. Dolor. 16, 147–152. doi: 10.1016/S1134-8046(09)71006-7
Trenti, G. F., and Gheza, G. (2002). Efficacy of oxygen-ozone pain therapy associated with shock waves to treat calcifying tendinitis of the shoulder. Preliminary findings. Riv. Ital. Ossigeno-Ozone Ther. 1, 45–50.
Vanni, D., Galzio, R., Kazakova, A., Pantalone, A., Sparvieri, A., Salini, V., et al. (2015). Intraforaminal ozone therapy and particular side effects: preliminary results and early warning. Acta Neurochir. 158, 491–496. doi: 10.1007/s00701-015-2545-y
Vilas-Rolan, D., Mila, M., Cuberas, G., Becerra, J. L., Herva, J. V., Massuet, A., et al. (2012). Neurological symptoms following exposure to ozone. J. Neurol. 259, 2740–2742. doi: 10.1007/s00415-012-6667-3
Wang, M. C., Chan, L., Maiman, D. J., Kreuter, W., and Deyo, R. A. (2007). Complications and mortality associated with cervical spine surgery for degenerative disease in the United States. Spine 32, 342–347. doi: 10.1097/01.brs.0000254120.25411.ae
Wen-Juan, T., Long, J., Ying, W., and Ze-Min, K. (2017). Ozone therapy induced sinus arrest in a hypertensive patient with chronic kidney disease: a case report. Medicine 96:e9265.
Xiao, Y. Y., Tian, J. L., Li, J. K., and Zhang, J. S. (2006). CT guided ozone injection for the treatment of cervical disc herniation. Riv. Ital. Ossigeno-Ozone Ther. 5, 109–115.
Yang, C. S., Zhang, L. J., Sun, Z. H., Yang, L., and Shi, F. D. (2018). Acute prevertebral abscess secondary to intradiscal oxygen–ozone chemonucleolysis for treatment of a cervical disc herniation. Int. J. Med. Res. 46, 2461–2465. doi: 10.1177/0300060518764186
Zambello, A., Fara, B., Tabaracci, G., and Bianchi, M. (2006). Epidural steroid injection vs paravertebral O2-O3 infiltration for symptomatic herniated disc refractory to conventional treatment: a prospective randomized study. Riv. Ital. Ossigeno-Ozone Ther. 5, 123–127.
Zanardi, G., and Zorandi, A. (2002). Ossigeno-ozone therapy in the treatment della painful pathology of nell’atleta foot. Riv. Ital. Ossigeno-Ozone Ther. 1, 51–56.
To date, the application of oxygen-ozone (O2O3) therapy has significantly increased in the common clinical practice in several pathological conditions. However, beyond the favorable clinical effects, the biochemical effects of O2O3 are still far from being understood. This comprehensive review aimed at investigating the state of the art about the effects of O2O3 therapy on pro-inflammatory cytokines serum levels as a modulator of oxidative stress in patients with musculoskeletal and temporomandibular disorders (TMD). The efficacy of O2O3 therapy could be related to the moderate oxidative stress modulation produced by the interaction of ozone with biological components. More in detail, O2O3 therapy is widely used as an adjuvant therapeutic option in several pathological conditions characterized by chronic inflammatory processes and immune overactivation. In this context, most musculoskeletal and temporomandibular disorders (TMD) share these two pathophysiological processes. Despite the paucity of in vivo studies, this comprehensive review suggests that O2O3 therapy might reduce serum levels of interleukin 6 in patients with TMD, low back pain, knee osteoarthritis and rheumatic diseases with a concrete and measurable interaction with the inflammatory pathway. However, to date, further studies are needed to clarify the effects of this promising therapy on inflammatory mediators and their clinical implications.
Ozone gas (O3) was discovered in 1840, and its expansion into the medical field has given rise to compelling research in the recent decades to validate its clinical value [1]. Despite some controversies, several papers [2,3,4,5,6,7,8,9,10,11] have proposed relevant medical features, including bactericidal and virucidal effects, inflammatory modulation and circulatory stimulation, with considerable applications in several medical fields such as wound healing, ischemic disorders, infections, and chronic inflammatory conditions such as musculoskeletal disorders.
The function of O3 shares similarities with that of a prodrug, as it is modified upon reacting with molecules to develop more active substrates, thus prompting an endogenous cascade of reactions [12]. On the other hand, it is hard to classify O3 as merely a prodrug, due to its power to directly interact with phospholipids, lipoproteins, bacteria envelopes and viral capsids. Therefore, O3 is considered one of the most powerful oxidizing molecules in nature, although, at high concentrations, it rapidly decomposes into ordinary oxygen [13]. O3 rapidly reacts with water and polyunsaturated fatty acids (PUFA) and in human fluids and tissues, producing, respectively, hydrogen peroxide (H2O2) and a combination of lipid ozonation products (LOP), mainly composed by 4-HNE (from omega-6 PUFA) and 4-HHE (trans-4 hydroxy-2-hexenal from omega-3 PUFA) [13]. In this context, H2O2, acting as an ozone messenger, is considered as the fundamental reactive oxygen species (ROS). However, other ROS have been identified as products of ozone reactions, such as superoxide ions and hydroxyl radical (OH−) [14]. Hence, given the role of signal transduction, the previous concept that ROS are always harmful has recently been revised and replaced by the latest evidence describing ROS as mediators of the host defense and immune responses [15].
Cytokines are undoubtedly involved in these processes and the proinflammatory cytokines tumor necrosis factor-α (TNF-α), interleukin-1 (IL-1), macrophage migration inhibitory factor (MIF) play a pivotal role [16,17]. Cytokines have been considered encouraging biomarkers and clinical targets in rheumatic and oncologic therapies, but, to date, anti-cytokine-based therapeutic approaches such as the use of anti-TNF antibodies, soluble TNF receptors or IL-1 receptor antagonists have failed to ascertain a clear clinical advantage [18,19]. In addition, some antioxidants and ROS scavengers could exert a protecting effort against endotoxic shock in rodents by hampering TNF-α.
Thus, it has been demonstrated that ozone–oxygen (O2O3) mixture might play a key role as a microbiocidal agent compared to the rich bactericidal activity of NO, serving as a modulator of several inflammatory processes in vivo [20,21]. O2O3 exhibits various effects on the immune system, such as the modulation of macrophages’ phagocytic activity, which provides the first-line defense against bacteria and toxins [22].
In this scenario, O2O3 concentrations should be set to a specific range to ensure safety; however, patients might present a sensation of heaviness at the injection site that spontaneously decreases in a few minutes. On the contrary, other adverse effects might be related to an incorrect administration technique, including vagal crisis, pain, hematoma in the injection site, local infections, and even death [23,24,25].
Moreover, it has been demonstrated that low amounts of ozone increased endogenous antioxidant pathways, entangling glutathione (GSH), superoxide dismutase (SOD) and catalase (CAT), and preparing the host to face ROS-mediated physiopathological circumstances. The ozone, through oxidative preconditioning, protects tissues from ROS-related damage, promoting the antioxidant–prooxidant balance and the concomitant preservation of the cell redox state [26,27,28]. Therefore, we could hypothesize that O2O3 mixture could enhance proinflammatory cytokine modulation [29].
Musculoskeletal disorders are considered as a common cause of pain and functional disability, predicting a burden that will further increase due to the aging of the population [30,31,32,33,34]. They include all inflammatory and rheumatic diseases affecting the osteoarticular system such as osteoarthritis (OA), but also low back pain and temporomandibular disorders [35,36,37,38,39].
O2O3 therapy has assumed the role of an adjuvant therapeutic approach in various pathological disorders characterized by chronic inflammatory processes and immune hyper activation, and most musculoskeletal disorders share these two pathophysiological scenarios [40]. In this context, several authors presented a practical function of O2O3 in the management of low back pain (LBP) with promising perspectives, as a minimally invasive approach, for the conservative therapies of disc herniation or protrusion and in case of failed back surgery syndrome [41,42,43,44,45,46,47]. At the same time, a recent systematic review [48] documented that knee pain could be decreased after O2O3 intra-articular management in patients affected by knee osteoarthritis (KOA). Likewise, tendon disorders are another conceivable focus for O2O3 therapy, and a recent randomized controlled trial (RCT) evaluated the usefulness of O2O3 therapy in patients with shoulder impingement, indicating that it might be assumed an intriguing alternative intervention in case of contraindication to corticosteroids [49]. Moreover, O2O3 injective treatment reported positive results after O2O3 injection in patients with lateral chronic epicondylitis not responding to conventional therapy [50]. Lastly, favourable developments have been documented even in rheumatic diseases, where O2O3 rectal insufflations or autohemotherapy seemed to reveal a profitable safety profile, promoting positive prospective in fibromyalgia [51].
A common denominator of these widespread pathologies is the low-grade inflammatory profile, with a similar serum pattern of inflammatory mediators [52,53,54]. This concept has been recently investigated for the development of more specific and sensitive methods for early diagnosis and follow-up, starting from a detailed and targeted phenotypic characterization of musculoskeletal and temporomandibular disorders [55].
To date, although it has been suggested that O2O3 therapy could be an effective analgesic treatment, its specific anti-inflammatory effects in terms of serum levels of cytokines modifications are controversial.
Several other musculoskeletal diseases might take advantage of the O2O3 therapy that is commonly used in the PRM clinical practice. However, only a few papers have investigated the effects of O2O3 therapy on other musculoskeletal disorders leading to disability (i.e., cervical pain, tendinopathies, and fibromyalgia). Moreover, it should be considered that O2O3 therapy is commonly used in the clinical practice as anti-inflammatory and analgesic therapeutic option for temporomandibular disorders (TMD) and general musculoskeletal and rheumatic diseases (Figure 1).
Main clinical targets for oxygen-ozone therapy as anti-inflammatory and analgesic treatment.
Therefore, in the present comprehensive review, we aimed to investigate the state of the art about the effects of O2O3 therapy on pro-inflammatory cytokines serum levels as a modulator of oxidative stress in patients with TMD and musculoskeletal disorders.
O3 is composed of three oxygen atoms with a cyclic structure [56]. It is generated for medical use from pure oxygen which passes through a high voltage gradient (5–13 mV) following the reaction:
3O2 + 68,400 cal → 2O3
The result is a gas mixture composed of not less than 95% oxygen and not more than 5% O3. O3 is 1.6 times denser and 10 times more soluble in water than oxygen. It should be considered that O3 is the most powerful oxidant after fluorine and persulfate, although it is not a radical molecule. It is an unstable gas that cannot be stored and should be used right away as it has a half-life of 40 min at 20 °C. Despite the heterogeneous and current applications in the medical field, the biochemical effects of O2O3 are still difficult to understand, even if its properties and chemical characteristics seem to suggest some of its positive clinical effects [40,44,57,58,59].
Like any other gas, O3 physically dissolves in pure water according to Henry’s law in relation to temperature, pressure, and ozone concentration. Unlike O2, O3 reacts immediately with the water present in the tissues. O3 reacts with polyunsaturated fatty acids (PUFA), antioxidants such as ascorbic and uric acid, and thiol compounds with -SH groups (cysteine, reduced glutathione-GSH and albumin). Depending on the dose of O3 administered, enzymes, carbohydrates, DNA and RNA may also be involved in the process. These compounds undergo oxidation, acting as electron donors [56]. O3, interacting with water and PUFA, present in the tissues, leads to the formation of hydrogen peroxide (H2O2), a fundamental reactive oxygen species (ROS) which acts as an ozone messenger, and other lipid ozonation products (LOPs) [33,34,35].
H2O2 is a non-radical oxidant capable of acting as an O3 messenger to elicit numerous biological and therapeutic effects. The fact that ROS are always harmful is a concept widely revised in the literature as, in physiological quantities, they are considered mediators of host defense and immune responses. Moreover, they have an extremely short duration (seconds), but by virtue of their reactivity, they could damage cellular components if their generation is not well calibrated. The composition of ROS in the plasma is very rapid and is accompanied by a transient (15–20 min for the recycling of oxidized compounds) and modest decrease in the antioxidant capacity. H2O2 diffuses very easily from plasma to cells (intracellular gradient 1/10 of the plasma one) and represents an important biological stimulus. In tissues, the moderate oxidative stress of ROS is canceled by endogenous radical scavengers (superoxide dismutase, glutathione peroxidase, catalase, NADPH quinone-oxidoreductase, etc.) [60,61].
An excess of ROS can in fact lead to the formation of toxic compounds such as peroxynitrite (O5NOO2) and hypochlorite anion (ClO2). Furthermore, the presence of traces of Fe++ should be avoided because, in the presence of hydrogen peroxide, they catalyze the formation of the most reactive OH, through the Fenton reaction (hydroxyl radical) [56].
LOPs (lipoperoxides-LOO, alkoxy radicals-LO, lipohydroperoxides-LOOH, iso-prostane and alkenes (4-hydroxy-2,3-transnonenal-HNE and malonyldialdehyde-MDA)) are signal molecules of acute oxidative stress and they cause an upregulation of antioxidant enzymes, such as superoxide dismutase (SOD), GSH-peroxidase (GSH-Px), GSH-reductase (GSH-Rd) and catalase (CAT), which play a key role in antioxidant defense. They also induce oxidative stress proteins, one of which is heme-oxygenase I (HO-1 or HSP-32), which degrades the heme molecule. Being toxic and much more stable in vitro than ROS, they must be generated in very low concentrations and metabolized by GSH-transferase (GSH-Tr) and aldehyde dehydrogenase [56].
Therefore, following the administration of O3 the formation of ROS and LOP takes place and, due to their chemical diversity, they act in two different phases. ROS behave as early and short-acting messengers, while on the other hand, LOPs act as late and long-lasting messengers. Thus, they spread in different tissues and bind in small quantities to cell receptors, thus minimizing their toxicity [56].
Small and repeated oxidative stresses might induce the activation of the transcriptional factor mediating nuclear factor-erythroid 2-related factor 2 (Nrf2), a domain involved in the transcription of antioxidant response elements (ARE) and usually bound to protein 1 associated with ECH Kelchlike (Keap-1), thus creating an inactive complex in the intracellular space. A mild oxidative stress can therefore favor the release of Nrf2 from this complex and its migration into the nucleus, where it would favor the transcription of different AREs on the DNA, binding to the Maf protein [62,63].
Therefore, through repeated mild oxidative stresses, O3 could induce the upregulation of Nrf2, conditioning human cells to transcribe different AREs, stimulating a better response to pathological radical stress, common in most chronic inflammatory diseases [12].
Several antioxidant enzymes reach a higher level of concentration in response to the production of AREs, such as superoxide dismutase, catalase (CAT), glutathione-transferase (GST), heme oxygenase (HO)-1, heat shock proteins, glutathione peroxidase and quinone-oxidoreductase. These enzymes play a “scavenger role” of free radicals. Based on the redox state of the cell and the amount of O2O3 administered, we can observe different effects. For example, O2O3 overexpresses HO-1 or NO-producing 32 kPa heat shock proteins (Hsp34) and, furthermore, Hsp70 expression levels are in turn upregulated by O2O3, which is related to HO-1. Heme is enzymatically degraded by HO-1 and can be toxic depending on free iron, amount produced and biliverdin. Biliverdin is a nitrosative and oxidative stress neutralizer based on the ability to interact with reactive nitrogen and NO species. The response to thermal shock provides a cytoprotective state during an inflammatory process, aging and neurodegenerative disorders. HO isoforms appear to be regulators of cellular redox homeostasis, functioning as dynamic sensors of its oxidative stress. O2O3 may play a role in regulating the proinflammatory and anti-inflammatory effects of prostaglandin formation, which is similar in nature to NO [40].
Furthermore, Nrf2 appears to play an important role in the intracellular signaling pathways of inflammation. Indeed, the activation of the Nrf2-antioxidant signal could attenuate a key regulator of the inflammatory response and muscle atrophy (NF-B), and furthermore, the literature suggests that the inflammatory response could be directly down-regulated by suppression of crucial inflammatory mediators and cytokines (IL-6, IL-8 and TNF-a) [64,65,66].
Low doses of O3 could therefore play a role in the regulation of prostaglandin synthesis, in the release of bradykinin and in the increase of macrophage and leukocyte secretions. It is widely accepted that pain is a common symptom related to the inflammatory process and O2O3 therapy could play a key role not only in the management of inflammation, but also in nociceptive perception and modulation. As for the analgesic use of O2O3, after the administration of O2O3, an increase in antioxidant molecules (serotonin and endogenous opioids) has been demonstrated, which would induce pain relief by stimulating the antinociceptive pathways [3,6,67,68,69].
Therefore, the effect of O3 mimics an acute oxidative stress that, if properly balanced, is not harmful, but is able to elicit positive biological responses and reverse chronic oxidative stress (degenerative process, aging, etc.) This hypothesis about ozone and oxidative stress modulation could be better defined as a “real non-toxic therapeutic shock able to restore homeostasis” [56,70,71].
Little evidence is available in literature about the effect of O2O3 injections in patients with low back pain due to lumbar disc herniation [72,73]. Although the fluoroscopy or tomography guide requirement could limit the feasibility of this therapy in conventional rehabilitation settings, positive effects were reported in comparison with other interventions such as steroid intraforaminal injection [74]. On the contrary, intramuscular-paravertebral O2O3 therapy seems to be safe, reliable, and effective to reduce pain in patients affected by LBP not responding to anti-inflammatory/analgesic drugs [75,76].
The O2O3 might exert its action combining mechanical and anti-inflammatory effects, breaking glycosaminoglycan chains in the nucleus pulposus, decreasing their capability to retain water, thus lowering the size of the herniated position, and allowing to relieve the hernial conflict [22,77]. A reduction in disk volume is the result of all these events. In a study conducted by Andreula et al. [78], five histologic disk specimens were removed during surgical microdiscectomy, providing intradiscal injections of O3 at 27 µg/mL, and reporting the nucleus pulposus fibrillary matrix dehydration, regression, and collagen fibers revealing. Parallelly, O2O3 might also influence the inflammatory cascade by modulating the breakdown of arachidonic acid into prostaglandins and facilitating the fibroblastic action, stimulating the deposition of collagen and the initiation of the repairing process at the tissue level [57].
Around the disc protrusion, inflammatory mediators prompted by granulation tissue are known to attract histiocytes, fibroblasts, and chondrocytes that can produce interleukin-1α (IL-1α), interleukin-6 (Il-6), and TNF-α; these cytokines induce the prostaglandin E2 pathway, which causes pain or increases the sensitivity of the nerve roots to other algogenic substances, such as bradykinin [79]. In vivo, local injection of medical ozone would increase the concentrations of TNF-α, IL1β, and IFN-γ around the disc, suggesting that the contact of medical ozone with the disc damages the extracellular matrix, resulting in shrinkage and decompression of the surrounding neurons. This might proceed probably together with the decrease in lactic acid and inflammatory cytokines, resulting in the decrease of low back pain and sciatica [80].
Furthermore, this disk shrinkage can enhance local microcirculation and increase oxygen supply by decreasing venous stasis caused by disk vessel compression. The O2O3 therapy might have analgesic and anti-inflammatory effects in treating disk herniation due to the neutralization of proinflammatory cytokines by boosting the surge of antagonists’ release [25].
When a disc degeneration leads to disc herniation, the adjacent nervous system structures, such as the nerve roots, or the dorsal root ganglion can be affected, causing neuropathic pain of mechanical or biochemical origin [81]. Moreover, other spinal structures are damaged, including facet joints, ligaments, and muscles, which can also become pain generators [82]. However, the peripheral sensitization should be avoided by O2O3 mediators, since recent evidence suggests that ozonized low-density lipoprotein inhibits NFkB and IL-1 receptor-associated kinase 1 (IRAK-1) signaling [83]. At the same time, the oxidation of IL, IL receptors, or nuclear factors might block COX-2 expression [84]. Clinically, Niu et al. showed that low concentrations of medical ozone (20 and 40 μg/mL) can reduce the serum IL-6, IgG, and IgM expression, presenting as analgesic and anti-inflammatory effects; while high concentrations of medical ozone (60 μg/mL) increase the serum IL-6, IgG, and IgM expression, presenting as pain and pro-inflammatory effects. Thus, the medical ozone concentration of 40 μg/mL seemed to report the optimal treatment efficacy [85].
In conclusion, ozone therapy might reduce the autoimmune inflammatory reaction and, consequently, pain due to radiculopathy, after the exposure of the nucleus pulposus to the immune system [22]. Intramuscular O2O3 therapy is a safe and widely used procedure in the common clinical practice but these results could be only achieved starting from strict eligibility criteria in patient selection and trained and experienced physicians to perform the procedure. Nevertheless, further research must provide evidence for a correct balance between O2O3 dosage and inflammatory mediators’ expression.
OA is a widespread musculoskeletal disease and a leading cause of chronic disability [86]. Conservative estimates state that up to 240 million people worldwide suffer from it [87]. OA is not merely a degenerative disease, considering that both mechanical and inflammatory factors are attributed to its pathophysiology [88,89,90]. The paradigm of OA is changing from the non-inflammatory theory of “wear and tear” to the hypothesis of “chronic low-grade inflammation” [91,92]. Long-time exposure to chronic low-grade inflammation and imbalance in oxidant-antioxidant systems is involved in OA pathogenesis and progression by compromising the complex network of signaling pathways that regulate cartilage and subchondral bone homeostasis [93,94].
A crucial role in this process might be played by inflammatory cytokines released by chondrocytes (IL-1β, IL-6, IL-8, IL-17, TNF-α, IFN-γ), promoting the catabolism of cartilage and subchondral bone [93,94]. Under normal conditions, these catabolic factors are in equilibrium with anabolic factors that include anti-inflammatory cytokines (IL-4, IL-10) and anabolic cytokines (TGF-β, IGF-1, FGF-18, and PDGF) [95,96,97]. Inflammatory and catabolic factors produce an imbalance that leads a healthy joint to develop OA [97].
As a result, clinical research is looking for immunomodulatory treatments that can act on inflammation to reduce the progression of OA and stimulate the synthesis of anabolic factors [48]. Among these, O2O3 represents a promising treatment option for its ability to modulate inflammation, promote cartilage growth, and joint repair mechanisms [48,61,98]. O3 might influence the modulation of inflammation through different mediators and signaling pathways [4,99,100]. In synovial fluid, O3 decreases the production of pro-inflammatory cytokines, particularly IL-6, IL-1β, and TNF-α, which are responsible for cartilage degradation [101]. This effect of ozone has been observed and demonstrated in several studies in animal models of knee OA (KOA), rheumatoid arthritis, and in models of ischemia/reperfusion, e.g., in the reduction of neuropathic pain [3,98,102].
A recent in vivo study on intra-articular O2O3 injection treatment in patients with KOA has shown that O3 is capable of reducing serum levels of IL-6 [91]. This is particularly interesting because IL-6 is produced by IL-1β and TNF-α, two important inflammatory cytokines that appear to play a key role in the initiation and development of OA [103]. IL-1 is responsible for cartilage destruction whereas TNF-α activates the inflammatory process [91]. The authors also demonstrated that O3 could be capable of improving serum IGF-1 levels. IGF-1 is a growth factor with important properties in reducing inflammation and stimulating cell growth, differentiation, and tissue repair [104].
Hashemi et al. obtained similar results showing that treatment with intra-articular injections of ozone in patients with KOA induces a significant reduction in serum levels of inflammatory cytokines at 1, 2, and 6 months after the procedure [101]. This result is also greater at 2 and 6 months compared with patients treated with steroid injections. Notably, IL-1b and TNF-α serum levels significantly decreased in the ozone group compared with the steroid group. The authors’ hypothesis is that ozone is likely to have a more stable anti-inflammatory effect than steroids. Although the steroid has a robust anti-inflammatory action against inflammatory cytokines, this effect in cartilage tissue was shorter than ozone. The biochemical findings of this study are also confirmed by the clinical outcomes; in fact, patients treated with ozone demonstrated a more lasting improvement in pain and disability compared to steroid injection.
These results represent in vivo confirmation of previous in vitro experiments focusing on the ability of ozone to reduce serum levels of pro-inflammatory cytokines by stimulating the production of anti-inflammatory cytokines and anabolic chemokines. These intriguing biological effects could be strictly connected to the clinical improvements observed in these patients.
Inflammatory cytokines can also increase the production of ROS which can activate the NF-Кβ pathway leading to accelerating cartilage matrix disintegration and apoptosis [105,106,107,108,109]. Ozone has been observed to decrease the NF-Кβ pathway and enhance the Nrf2 (Nuclear factor erythroid 2-related factor 2) pathway, which is involved in the generation of antioxidant response elements (AREs) such as superoxide dismutase (SOD), catalase (CAT), glutathione peroxidase (GPx), and hemoxygenase-1(HO-1) [110,111]. The activated NF-Кβ pathway could lead to a downstream cascade of other proinflammatory cytokines giving rise to a vicious circle that perpetuates the chronic inflammatory process [112]. Ozone inhibition of NF-Кβ activation can reduce the degradation of the cartilage matrix and initiation of the apoptotic pathway, thus supporting cell survival [108] (Figure 2).
Ozone (O3) intracellular and intranuclear pathways involved in inflammation and oxidative stress.
Although injured or damaged articular cartilage remains one of the most difficult tissues to treat [113], it has been recently highlighted that the ozone could provide promising results as a safe and effective treatment in patients with KOA from both a biochemical and clinical perspective [3,114,115,116,117,118,119,120,121].
Rheumatoid arthritis (RA) is the most frequent pathology associated with chronic joint inflammation, a genetic degenerative disease that initially affects extremity joints and is characterized by a chronic inflammatory state that distorts and demolishes articular cartilage and expands connective tissue fibrosis, leading to cell destruction and subchondral bone deterioration. It has been estimated that about 1% of the world population suffers from this disorder [122]. O2O3 therapy effectively decreased inflammation with a down-regulation of pro-inflammatory cytokines and an up-regulation of IL-10 anti-inflammatory cytokine [123]. Rajesh and collaborators investigated the temporal expression of cytokines during the initial phase of an experimental model of arthritic inflammation and revealed that interferon-gamma (IFN-γ) participates in inflammatory process modulation [124]. The O3 has also been shown to effectively increase the clinical response of methotrexate (MTX) in patients with rheumatoid arthritis induced by PG/PS. The combination therapy diminishes inflammation through reduction of IL-1B and TNF-α and decreases oxidative stress by reducing hydrogen and preventing damage to proteins and lipids [125].
In this scenario, O2O3 therapy seems to play a positive role in several inflammatory conditions due to its bacteriostatic, oxidative stress, immune and epigenetic modulation. Compared with topical ozone administration, systematic ozone therapy has apparent advantages in enhancing metabolism, blood hypercoagulability, angiosclerosis, insomnia, and rejuvenation of the body [2,126]. Thus, psoriasis vulgaris is a chronic immune-mediated inflammatory cutaneous disease characterized by red, itchy, and scaly skin patches. Patients typically suffer disfiguration, disability, and associated comorbidities [112]. Zeng et al. indicated that short-term O2O3 therapy seemed to attenuate psoriatic disease severity lowering the level of blood lipids and up-streaming PPAR-γ level in CD4 T cells, considering that the PPAR-γ expression is commonly reduced in CD4 T cells in psoriasis [127].
Systemic sclerosis (SSc) is an immune-mediated rheumatic disease, characterized by skin and visceral organs fibrosis and vasculopathy [128,129]. Carpal tunnel syndrome (CTS) is one of the most common entrapment disorders in general and the most recurring peripheral nervous system involvement in SSc [130,131]. Elawamy et al. demonstrated that both intracarpal ozone or methylprednisolone reported advantageous impacts upon CTS in people with SSC; nonetheless, ozone relieves pain, enhances the hand functioning, decreases the duration and frequency of Raynaud’s attacks, declines the size of ulceration, and improves median nerve conduction study over the 6-month follow-up [132]. Rascaroli et al. found slight improvements in sensory and motor parameters after ozone therapy, and Bahrami et al. showed improvement of median sensory nerve action potential latency, compared to the pre-treatment level in both groups (one group treated with wrist volar splint alone, the other group treated with ozone injection and splint) [133,134,135,136]. The nature of the fibrotic expression in SSc people with CTS seemed to be significantly associated with gene upstream for Col1 and Col3, TGF-β, and SMAD3 in CTS fibroblasts [137,138]. These studies, focusing on TGF-β signaling inhibition in CTS, reported that therapies targeted for the TGF-β pathway might eventually have utility for the prevention and treatment of CTS, as well as the anti-fibrotic effect of relaxin [137,138].
Gout disease is one of the most frequent causes of inflammatory arthritis in adults and is chronic disorder associated with self-limiting acute gout attacks (gout flare), caused by the accretion of monosodium urate (MSU) depositions in joints and surrounding soft tissue and bursa [139,140,141]. Acute episodes of gout disease are one of the most influential reasons for unfavourable health-related quality of life [139,140,141]. In a rat model, ozone therapy indicated a decrease in the degree of edematous ankle swelling, pro-inflammatory cytokines, lipid peroxidation, the nucleotide-binding oligomerization domain-like receptor containing pyrin domain 3 (NLRP3), procaspase-1, caspase-1, interleukin-1β synovial tissue levels with an enhancement of antioxidant defence system [142]. In other murine models, Bilge et al. demonstrated that ozone therapy raises the levels of antioxidant enzymes, including oxidative shock proteins (hemo-oxygenase-1), Interleukin 4 and Interleukin 10, TGF-β, NO endorphin, adrenocorticotropic hormone (ACTH), and cortisol levels [141].
In conclusion, the positive effect of ozone treatment sustained by its bidirectional regulation of immunity are present also in rheumatic diseases patients. These positive effects could be caused by a O2O3-related massive production of inflammatory modulation cytokines by immune cells.
Temporomandibular disorders (TMD) represent heterogeneous musculoskeletal disorders, defined as a multifactorial set of signs and symptoms involving masticatory muscles of the stomatognathic system, temporomandibular joint (TMJ), or both [143].
According to the Diagnostic Criteria for TMD (DC/TMD) Axis I, TMD could be divided in muscle disorders (including myofascial pain) or intra-articular disorders (including disc displacement with or without reduction, arthralgia, and arthritis) [144,145].
TMD are the second most common musculoskeletal disorders, affecting approximately 90% of the general population [146,147,148]. Indeed, TMD are the first most common cause of pain of non-dental origin in the maxillofacial region [149], with an incidence rate of 3.9% per annum [150].
Main clinical symptoms are pain and limited jaw range of motion, often accompanied by decrease in the maximal interincisal opening, muscle or joint tenderness on palpation, joint sounds, and otologic complaints (e.g., tinnitus, vertigo, or ear fullness) [151,152]. These signs and symptoms could lead to discomfort or difficulty in performing activities of daily living, such as eating, chewing, talking, swallowing, yawning, causing disability with a significantly reduced quality of life [153,154,155].
The etiology has been accepted as multifactorial, and parafunctional habits, clenching of teeth, grinding, as well as psychosocial issues, including anxiety depression are generally believed to contribute to the development or perpetuation of the pain complaints [156,157,158,159].
In response to this imbalance of the masticatory system, cytokines such as TNFα, IL-1, IL-6 and IL-8 are released within TMJ [160], thus promoting the release of proteinases and stimulating the expression of degrading enzymes and inflammatory mediators; all this mechanism could lead to a TMJ inflammation and bone and cartilage degradation [161]. Other cytokines and metallo-proteinases (MMPs) could be involved in the inflammatory process, including interferon-gamma (IFN-γ), prostaglandin E2 (PGE2), IL-17, MMP-2, MMP-9, aggrecanase-1 and aggrecanase-2 [162,163,164,165].
More in detail, both immune and non-immune cells could release TNF-α (e.g., macrophages, synoviocytes, and neurons associated with the trigeminal ganglion), causing TMJ inflammation and pain in myofascial TMD patients [165]. Ulmner et al. [166] characterized and quantified the synovial tissue cytokines and related the result to the diagnoses of disc displacement with or without reduction. Results of this study showed that bone morphogenetic protein (BMP) type 2 and 4, epidermal growth factor (EGF), eotaxin, granulocyte-colony stimulating factor (G-CSF), IL-1β, IL-7, IL-8, IL-10, macrophage inflammatory protein (MIP) 1β, TNF-α and TNF-β had significantly higher concentrations in patients with disc displacement without reduction. In 2021, Son et al. [167] investigated the relationship between long-term clinical characteristics and different cytokine and autoimmunity levels in young female TMD patients according to pain disability. The subjects included in the study were classified in high and low disability groups, according to the Graded Chronic Pain Scale (GCPS). The authors showed that IL-8 and IgG levels were significantly higher in the high disability group (p = 0.047 and 0.005, respectively).
Several conservative treatments have been used for reducing TMD-related pain, including occlusal splint devices [168,169], behavioral therapies [170], manual therapy [171], laser therapy [172], transcutaneous electrical nerve stimulation (TENS) [173], dry needling [173]. In this context, O2O3 therapy [152,174,175,176] might be considered as a promising new treatment to reduce TMD pain, although the mechanism of action should still be adequately investigated [177]. Probably, O2O3 might effectively decrease inflammation with a down-regulation of pro-inflammatory cytokines and an up-regulation of IL-10 anti-inflammatory cytokine [123].
In the context of muscle-related TMD, Celakil et al. [178] recently conducted a double-blind randomized clinical trial in order to evaluate the efficacy of ozone therapy compared to placebo. Topical gaseous ozone therapy was applied to the muscles of 20 participants three times per week for 10 min for 2 weeks, with a significantly lower VAS score than placebo group after treatment (p = 0.040). Moreover, the pressure pain threshold of the temporal muscle, masseter muscle, and TMJ lateral pole were significantly higher in the ozone group (p = 0.035; p = 0.007; p = 0.012, respectively). The same authors also compared the bio-oxidative ozone therapy to occlusal splints therapy in patients affected by both muscle and articular TMD disorders [135,175,179], showing that both therapies were effective in the improvement of mandibular movements and VAS scores. However, evaluating the effects in terms of PPT measurement of the temporal and masseter, their results indicated that occlusal splint treatment produced better results than ozone application (p = 0.046; p = 0.024, respectively). In the context of intra-articular TMD, Daif et al. compared the effects of TMJ ozone injections to medication therapy in TMD patients with disc displacement with reduction [180]. In the ozone group, each joint received 2 mL ozone–oxygen mixture (10 μg/mL) injections, 2 times per week for 3 weeks, whereas patients in the second group received nonsteroidal anti-inflammatory drugs and muscle relaxants showing. Results of this study showed that 87% of the patients who received ozone gas injections into the superior joint space either completely recovered (37%) or improved (50%), whereas in the medication group, only 33% of the patients showed an improvement in their clinical dysfunction indexes.
To date, the precise mechanism underpinning the positive effects of O2O3 therapy in TMD patients are far from being understood. However, O3 decreases the production of pro-inflammatory cytokines, particularly IL-6, IL-1β, and TNF-α, which are responsible for cartilage degradation in the synovial fluid [101]. Thus, when injected into a joint capsule, O2O3 could be able to stimulate the intrinsic fibroblastic joint repairing abilities and to promote new cartilage growth as well as reducing inflammation [180,181]. Therefore, ozone therapy is a not-invasive, fast, and comfortable treatment modality that seems to be effective in the pain management framework in TMD. This could have positive implications for these patients in improving mandibular function, although the precise role of O2O3 on serum levels of pro-inflammatory cytokines should be better investigated.
In conclusion, this comprehensive review describes the impact of O2O3 therapy on serum cytokine levels in different settings and conditions. As previously described, musculoskeletal and rheumatological disorders include several pathological conditions characterized by different and complex therapeutic approaches. In this scenario, O2O3 therapy remains a promising conservative and minimally invasive intervention that improves pain symptoms and patients’ quality of life. To date, evidence suggests a role of O2O3 therapy in IL-6 and IL-10 serum level modulation, although the precise epigenetic mechanism remains controversial. Therefore, further high-quality studies are needed to fully understand the molecular, epigenetic, and biochemical effects of O2O3 and its therapeutic implications.
Conceptualization, A.d.S.; methodology, A.d.S.; formal analysis, N.M., M.F., F.A., C.S., and L.L.; data curation, A.d.S., S.R., A.G., M.I. and A.A.; writing—original draft preparation, A.d.S. and N.M.; writing—review and editing, M.I. and A.A.; visualization, M.F., F.A., C.S., L.L., S.R. and A.G.; supervision, A.d.S. All authors have read and agreed to the published version of the manuscript.
1. Di Meo S., Venditti P. Evolution of the Knowledge of Free Radicals and Other Oxidants. Oxid. Med. Cell. Longev. 2020;2020:9829176. doi: 10.1155/2020/9829176. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
2. Akkawi I. Ozone therapy for musculoskeletal disorders: Current concepts. Acta Biomed. 2020;91:e2020191. doi: 10.26717/BJSTR.2019.22.003737. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
3. de Sire A., Stagno D., Minetto M.A., Cisari C., Baricich A., Invernizzi M. Long-term effects of intra-articular oxygen-ozone therapy versus hyaluronic acid in older people affected by knee osteoarthritis: A randomized single-blind extension study. J. Back Musculoskelet. Rehabil. 2020;33:347–354. doi: 10.3233/BMR-181294. [PubMed] [CrossRef] [Google Scholar]
4. Apuzzo D., Giotti C., Pasqualetti P., Ferrazza P., Soldati P., Zucco G.M. An observational retrospective/horizontal study to compare oxygen-ozone therapy and/or global postural re-education in complicated chronic low back pain. Funct. Neurol. 2014;29:31–39. doi: 10.11138/FNeur/2014.29.1.031. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
5. Galiè M., Covi V., Tabaracci G., Malatesta M. The role of Nrf2 in the antioxidant cellular response to medical ozone exposure. Int. J. Mol. Sci. 2019;20:4009. doi: 10.3390/ijms20164009. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
6. Paoloni M., Di Sante L., Cacchio A., Apuzzo D., Marotta S., Razzano M., Franzini M., Santilli V. Intramuscular oxygen-ozone therapy in the treatment of acute back pain with lumbar disc herniation: A multicenter, randomized, double-blind, clinical trial of active and simulated lumbar paravertebral injection. Spine. 2009;34:1337–1344. doi: 10.1097/BRS.0b013e3181a3c18d. [PubMed] [CrossRef] [Google Scholar]
7. Baranova I.V., Bezsmertnyi Y.A., Bezsmertnaya H.V., Postovitenko K.P., Iliuk I.A., Gumeniuk A.F. Analgetic effect of ozone therapy: Myths of reality? Pol. Ann. Med. 2020;27:62–67. doi: 10.29089/2020.20.00099. [CrossRef] [Google Scholar]
8. Rajkumar K.V., Jeevitha M., Sangeetha S. Knowledge and awareness of ozone therapy among dental professionals. Int. J. Res. Pharm. Sci. 2020;11:303–307. doi: 10.26452/ijrps.v11iSPL3.2931. [CrossRef] [Google Scholar]
9. Fitzpatrick E., Holland O.J., Vanderlelie J.J. Ozone therapy for the treatment of chronic wounds: A systematic review. Int. Wound J. 2018;15:633–644. doi: 10.1111/iwj.12907. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
10. Sanjeevi J., Santhosh Kumar M.P. Ozone therapy in dentistry. Drug Invent. Today. 2019;12:154–157. doi: 10.15274/inr-2014-10083. [CrossRef] [Google Scholar]
11. Masan J., Sramka M., Rabarova D. The possibilities of using the effects of ozone therapy in neurology. Neuroendocrinol. Lett. 2021;42:13–21. [PubMed] [Google Scholar]
12. Smith N., Wilson A., Gandhi J., Vatsia S., Khan S. Ozone therapy: An overview of pharmacodynamics, current research, and clinical utility. Med. Gas Res. 2017;7:212–219. doi: 10.4103/2045-9912.215752. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
13. Rajendran L., Knölker H.J., Simons K. Subcellular targeting strategies for drug design and delivery. Nat. Rev. Drug Discov. 2010;9:29–42. doi: 10.1038/nrd2897. [PubMed] [CrossRef] [Google Scholar]
14. Li Y.R., Trush M. Defining ROS in Biology and Medicine. React. Oxyg. Species. 2016;1:9–21. doi: 10.20455/ros.2016.803. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
15. Dumas A., Knaus U.G. Raising the ‘Good’ Oxidants for Immune Protection. Front. Immunol. 2021;12:42. doi: 10.3389/fimmu.2021.698042. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
16. Liu M., Xie Z., Sun G., Chen L., Qi D., Zhang H., Xiong J., Furey A., Rahman P., Lei G., et al. Macrophage migration inhibitory factor may play a protective role in osteoarthritis. Arthritis Res. Ther. 2021;23:59. doi: 10.1186/s13075-021-02442-w. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
17. Kany S., Vollrath J.T., Relja B. Cytokines in inflammatory disease. Int. J. Mol. Sci. 2019;20:6008. doi: 10.3390/ijms20236008. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
19. Gubernatorova E.O., Namakanova O.A., Gorshkova E.A., Medvedovskaya A.D., Nedospasov S.A., Drutskaya M.S. Novel Anti-Cytokine Strategies for Prevention and Treatment of Respiratory Allergic Diseases. Front. Immunol. 2021;12:1842. doi: 10.3389/fimmu.2021.601842. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
20. Malferrari M., Becconi M., Rapino S. Electrochemical monitoring of reactive oxygen/nitrogen species and redox balance in living cells. Anal. Bioanal. Chem. 2019;411:4365–4374. doi: 10.1007/s00216-019-01734-0. [PubMed] [CrossRef] [Google Scholar]
21. Vaneev A.N., Gorelkin P.V., Garanina A.S., Lopatukhina H.V., Vodopyanov S.S., Alova A.V., Ryabaya O.O., Akasov R.A., Zhang Y., Novak P., et al. In Vitro and in Vivo Electrochemical Measurement of Reactive Oxygen Species after Treatment with Anticancer Drugs. Anal. Chem. 2020;92:8010–8014. doi: 10.1021/acs.analchem.0c01256. [PubMed] [CrossRef] [Google Scholar]
22. de lo Erario M.Á., Croce E., Moviglia Brandolino M.T., Moviglia G., Grangeat A.M. Ozone as modulator of resorption and inflammatory response in extruded nucleus pulposus herniation. Revising concepts. Int. J. Mol. Sci. 2021;22:9946. doi: 10.3390/ijms22189946. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
23. Santos G.M., Pacheco R.L., Bussadori S.K., Santos E.M., Riera R., de Oliveira Cruz Latorraca C., Mota P., Benavent Caldas Bellotto E.F., Martimbianco A.L.C. Effectiveness and Safety of Ozone Therapy in Dental Caries Treatment: Systematic Review and Meta-analysis. J. Evid. Based. Dent. Pract. 2020;20:101472. doi: 10.1016/j.jebdp.2020.101472. [PubMed] [CrossRef] [Google Scholar]
24. Del Valle L.G., Guerra M.M.D., Carballo-Reyes A.L., Márquez J.A.S., Fernández O.E.L., Betancourt F.F., Zamora-Rodríguez Z., García L.A.F., Iznaga R.S., Casanueva R.M., et al. Observance of adverse reactions and analysis of biosafety compliance in the rectal application of ozone therapy in COVID-19 Cuban patients with acute infection or convalescent. J. Pharm. Pharmacogn. Res. 2021;9:465–473. [Google Scholar]
25. Bocci V. OZONE. Springer; Dordrecht, The Netherlands: 2010. The Clinical Application of Ozonetherapy. [Google Scholar]
26. Sharifi-Rad M., Anil Kumar N.V., Zucca P., Varoni E.M., Dini L., Panzarini E., Rajkovic J., Tsouh Fokou P.V., Azzini E., Peluso I., et al. Lifestyle, Oxidative Stress, and Antioxidants: Back and Forth in the Pathophysiology of Chronic Diseases. Front. Physiol. 2020;11:694. doi: 10.3389/fphys.2020.00694. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
27. Rao X., Zhong J., Brook R.D., Rajagopalan S. Effect of Particulate Matter Air Pollution on Cardiovascular Oxidative Stress Pathways. Antioxid. Redox Signal. 2018;28:797–818. doi: 10.1089/ars.2017.7394. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
28. Hasanuzzaman M., Bhuyan M.H.M.B., Zulfiqar F., Raza A., Mohsin S.M., Al Mahmud J., Fujita M., Fotopoulos V. Reactive oxygen species and antioxidant defense in plants under abiotic stress: Revisiting the crucial role of a universal defense regulator. Antioxidants. 2020;9:681. doi: 10.3390/antiox9080681. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
29. Franzini M., Valdenassi L., Ricevuti G., Chirumbolo S., Depfenhart M., Bertossi D., Tirelli U. Oxygen-ozone (O2-O3) immunoceutical therapy for patients with COVID-19. Preliminary evidence reported. Int. Immunopharmacol. 2020;88:106879. doi: 10.1016/j.intimp.2020.106879. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
30. Ruiz-Fernández C., Francisco V., Pino J., Mera A., González-Gay M.A., Gómez R., Lago F., Gualillo O. Molecular relationships among obesity, inflammation and intervertebral disc degeneration: Are adipokines the common link? Int. J. Mol. Sci. 2019;20:2030. doi: 10.3390/ijms20082030. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
31. Farrell S.F., de Zoete R.M.J., Cabot P.J., Sterling M. Systemic inflammatory markers in neck pain: A systematic review with meta-analysis. Eur. J. Pain. 2020;24:1666–1686. doi: 10.1002/ejp.1630. [PubMed] [CrossRef] [Google Scholar]
32. Blüher M. Inflammation: Between obesity, diabetes and exercise. Diabetologe. 2021;17:141–148. doi: 10.1007/s11428-021-00719-x. [CrossRef] [Google Scholar]
33. Paradis M.E., Couture P., Gigleux I., Marin J., Vohl M.C., Lamarche B. Impact of systemic enzyme supplementation on low-grade inflammation in humans. PharmaNutrition. 2015;3:83–88. doi: 10.1016/j.phanu.2015.04.004. [CrossRef] [Google Scholar]
34. Mobasheri A., Henrotin Y. Biomarkers of (osteo)arthritis. Biomarkers. 2015;20:513–518. doi: 10.3109/1354750X.2016.1140930. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
35. Ogura T., Suzuki M., Sakuma Y., Yamauchi K., Orita S., Miyagi M., Ishikawa T., Kamoda H., Oikawa Y., Kanisawa I., et al. Differences in levels of inflammatory mediators in meniscal and synovial tissue of patients with meniscal lesions. J. Exp. Orthop. 2016;3:7. doi: 10.1186/s40634-016-0041-9. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
36. Rahmati M., Mobasheri A., Mozafari M. Inflammatory mediators in osteoarthritis: A critical review of the state-of-the-art, current prospects, and future challenges. Bone. 2016;85:81–90. doi: 10.1016/j.bone.2016.01.019. [PubMed] [CrossRef] [Google Scholar]
37. Yucel-Lindberg T., Båge T. Inflammatory mediators in the pathogenesis of periodontitis. Expert Rev. Mol. Med. 2013;15:e7. doi: 10.1017/erm.2013.8. [PubMed] [CrossRef] [Google Scholar]
38. Tang C., Chen Y., Huang J., Zhao K., Chen X., Yin Z., Heng B.C., Chen W., Shen W. The roles of inflammatory mediators and immunocytes in tendinopathy. J. Orthop. Transl. 2018;14:23–33. doi: 10.1016/j.jot.2018.03.003. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
39. Abdulkhaleq L.A., Assi M.A., Abdullah R., Zamri-Saad M., Taufiq-Yap Y.H., Hezmee M.N.M. The crucial roles of inflammatory mediators in inflammation: A review. Vet. World. 2018;11:627–635. doi: 10.14202/vetworld.2018.627-635. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
40. Seyam O., Smith N.L., Reid I., Gandhi J., Jiang W., Khan S.A. Clinical utility of ozone therapy for musculoskeletal disorders. Med. Gas Res. 2018;8:103–110. [PMC free article] [PubMed] [Google Scholar]
41. Bonetti M., Zambello A., Princiotta C., Pellicanò G., Della Gatta L., Muto M. Non-discogenic low back pain treated with oxygen-ozone: Outcome in selected applications. J. Biol. Regul. Homeost. Agents. 2020;34:21–30. [PubMed] [Google Scholar]
42. Han H.J., Kim J.Y., Jang H.Y., Lee B., Yoon J.H., Jang S.K., Choi S.H., Jeong S.W. Fluoroscopic-guided intradiscal oxygen-ozone injection therapy for thoracolumbar intervertebral disc herniations in dogs. In Vivo. 2007;21:609–613. [PubMed] [Google Scholar]
43. Migliorini F., Maffulli N., Eschweiler J., Bestch M., Tingart M., Baroncini A. Ozone injection therapy for intervertebral disc herniation. Br. Med. Bull. 2020;136:88–106. doi: 10.1093/bmb/ldaa032. [PubMed] [CrossRef] [Google Scholar]
44. Melchionda D., Milillo P., Manente G., Stoppino L., Macarini L. Treatment of radiculopathies: A study of efficacy and tollerability of paravertebral oxygen-ozone injections compared with pharmacological anti-inflammatory treatment. J. Biol. Regul. Homeost. Agents. 2012;26:467–474. [PubMed] [Google Scholar]
45. Dal Fior S., Gaido C., Carnino I., Gamna F., Busso C., Massazza G., Minetto M.A. Clinical predictors of response to ozone therapy for treatment of discogenic and non-discogenic low back pain. J. Biol. Regul. Homeost. Agents. 2020;34:1223–1228. doi: 10.23812/19-564-L-36. [PubMed] [CrossRef] [Google Scholar]
46. de Magalhães F.N.O., Soares S.C., Torres J.M., Ungaretti A., Cacciacarro M.F., Teixeira M.J., Fonoff E.T. Effects of ozone applied by spinal endoscopy in patients with chronic pain related to failed back surgery syndrome: A pilot study. Neuropsychiatr. Dis. Treat. 2013;9:1759–1766. doi: 10.2147/NDT.S48663. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
47. Barbosa D.C., Ângelos J.S., De Macena G.M.J., De Oliveira Magalhães F.N., Fonoff E.T. Effects of ozone on the pain and disability in patients with failed back surgery syndrome. Rev. Assoc. Med. Bras. 2017;63:355–360. doi: 10.1590/1806-9282.63.04.355. [PubMed] [CrossRef] [Google Scholar]
48. Sconza C., Respizzi S., Virelli L., Vandenbulcke F., Iacono F., Kon E., Di Matteo B. Oxygen–Ozone Therapy for the Treatment of Knee Osteoarthritis: A Systematic Review of Randomized Controlled Trials. Arthrosc. J. Arthrosc. Relat. Surg. 2020;36:277–286. doi: 10.1016/j.arthro.2019.05.043. [PubMed] [CrossRef] [Google Scholar]
49. Travagli V., Zanardi I., Bernini P., Nepi S., Tenori L., Bocci V. Effects of ozone blood treatment on the metabolite profile of human blood. Int. J. Toxicol. 2010;29:165–174. doi: 10.1177/1091581809360069. [PubMed] [CrossRef] [Google Scholar]
50. Gökhan Ulusoy R., Bilge A., Öztürk Ö. Comparison of corticosteroid injection and ozone injection for relief of pain in chronic lateral epicondylitis. Acta Orthop. Belg. 2019;85:317–324. [PubMed] [Google Scholar]
51. Moreno-Fernández A.M., Macías-García L., Valverde-Moreno R., Ortiz T., Fernández-Rodríguez A., Moliní-Estrada A., De-Miguel M. Autohemotherapy with ozone as a possible effective treatment for Fibromyalgia. Acta Reumatol. Port. 2019;44:244–249. [PubMed] [Google Scholar]
52. Storheim K., Zwart J.A. Musculoskeletal disorders and the Global Burden of Disease study. Ann. Rheum. Dis. 2014;73:949–950. doi: 10.1136/annrheumdis-2014-205327. [PubMed] [CrossRef] [Google Scholar]
53. Minetto M.A., Giannini A., McConnell R., Busso C., Torre G., Massazza G. Common musculoskeletal disorders in the elderly: The star triad. J. Clin. Med. 2020;9:1216. doi: 10.3390/jcm9041216. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
54. Mendes A.F., Cruz M.T., Gualillo O. Editorial: The Physiology of Inflammation—The Final Common Pathway to Disease. Front. Physiol. 2018;9:1741. doi: 10.3389/fphys.2018.01741. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
55. Berenbaum F., Walker C. Osteoarthritis and inflammation: A serious disease with overlapping phenotypic patterns. Postgrad. Med. 2020;132:377–384. doi: 10.1080/00325481.2020.1730669. [PubMed] [CrossRef] [Google Scholar]
56. Bocci V.A. Scientific and medical aspects of ozone therapy. State of the art. Arch. Med. Res. 2006;37:425–435. doi: 10.1016/j.arcmed.2005.08.006. [PubMed] [CrossRef] [Google Scholar]
57. de Sire A., Agostini F., Lippi L., Mangone M., Marchese S., Cisari C., Bernetti A., Invernizzi M. Oxygen–ozone therapy in the rehabilitation field: State of the art on mechanisms of action, safety and effectiveness in patients with musculoskeletal disorders. Biomolecules. 2021;11:356. doi: 10.3390/biom11030356. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
58. Bernetti A., Agostini F., de Sire A., Mangone M., Tognolo L., Di Cesare A., Ruiu P., Paolucci T., Invernizzi M., Paoloni M. Neuropathic pain and rehabilitation: A systematic review of international guidelines. Diagnostics. 2021;11:74. doi: 10.3390/diagnostics11010074. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
59. de Sire A., Baricich A., Minetto M.A., Cisari C., Invernizzi M. Low back pain related to a sacral insufficiency fracture: Role of paravertebral oxygen-ozone therapy in a paradigmatic case of nociplastic pain. Funct. Neurol. 2019;34:119–122. [PubMed] [Google Scholar]
60. İnal M., Dokumacioglu A., Özcelik E., Ucar O. The effects of ozone therapy and coenzyme Q 10 combination on oxidative stress markers in healthy subjects. Ir. J. Med. Sci. 2011;180:703–707. doi: 10.1007/s11845-011-0675-7. [PubMed] [CrossRef] [Google Scholar]
61. Manoto S.L., Maepa M.J., Motaung S.K. Medical ozone therapy as a potential treatment modality for regeneration of damaged articular cartilage in osteoarthritis. Saudi J. Biol. Sci. 2018;25:672–679. doi: 10.1016/j.sjbs.2016.02.002. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
62. Sagai M., Bocci V. Mechanisms of action involved in ozone therapy: Is healing induced via a mild oxidative stress? Med. Gas Res. 2011;1:1–18. doi: 10.1186/2045-9912-1-29. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
63. Thi Xuan N., Hai Ha N., Thanh Chung D. Vitamin E Attenuates FasL-Induced Apoptotic Death of Dendritic Cells Through PI3K Signalling. VNU J. Sci. Med. Pharm. Sci. 2021;37:4268. doi: 10.25073/2588-1132/vnumps.4268. [CrossRef] [Google Scholar]
64. Mourkioti F., Kratsios P., Luedde T., Song Y.H., Delafontaine P., Adami R., Parente V., Bottinelli R., Pasparakis M., Rosenthal N. Targeted ablation of IKK2 improves skeletal muscle strength, maintains mass, and promotes regeneration. J. Clin. Investig. 2006;116:2945–2954. doi: 10.1172/JCI28721. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
65. Xie T., Yan W., Lou J., Chen X. Effect of ozone on vascular endothelial growth factor (VEGF) and related inflammatory cytokines in rats with diabetic retinopathy. Genet. Mol. Res. 2016;15:15027558. doi: 10.4238/gmr.15027558. [PubMed] [CrossRef] [Google Scholar]
66. Peralta C., León O., Xaus C., Prats N., Jalil E., Planell E.S., Puig-Parellada P., Gelpí E., Roselló-Catafau J. Protective effect of ozone treatment on the injury associated with hepatic ischemia-reperfusion: Antioxidant-prooxidant balance. Free Radic. Res. 1999;31:191–196. doi: 10.1080/10715769900300741. [PubMed] [CrossRef] [Google Scholar]
67. Peralta C., Xaus C., Bartrons R., Leon O.S., Gelpi E., Rosello-Catafau J. Effect of ozone treatment on reactive oxygen species and adenosine production during hepatic ischemia-reperfusion. Free Radic. Res. 2000;33:595–605. doi: 10.1080/10715760000301121. [PubMed] [CrossRef] [Google Scholar]
68. Paolucci T., Cardarola A., Colonnelli P., Ferracuti G., Gonnella R., Murgia M., Santilli V., Paoloni M., Bernetti A., Agostini F., et al. Give me a kiss! An integrative rehabilitative training program with motor imagery and mirror therapy for recovery of facial palsy. Eur. J. Phys. Rehabil. Med. 2020;56:58–67. doi: 10.23736/S1973-9087.19.05757-5. [PubMed] [CrossRef] [Google Scholar]
69. Longas Vélez B.P. Ozone therapy, a supplement for patients with fibromyalgia. Rev. Esp. Ozonoter. 2014;4:39–49. [Google Scholar]
70. Paolucci T., Agostini F., Bernetti A., Paoloni M., Mangone M., Santilli V., Pezzi L., Bellomo R.G., Saggini R. Integration of focal vibration and intra-articular oxygen–ozone therapy in rehabilitation of painful knee osteoarthritis. J. Int. Med. Res. 2021;49:6705. doi: 10.1177/0300060520986705. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
71. Agostini F., Bernetti A., Di Giacomo G., Viva M.G., Paoloni M., Mangone M., Santilli V., Masiero S. Rehabilitative Good Practices in the Treatment of Sarcopenia. Am. J. Phys. Med. Rehabil. 2020;100:280–287. doi: 10.1097/PHM.0000000000001572. [PubMed] [CrossRef] [Google Scholar]
72. Biazzo A., Corriero A.S., Confalonieri N. Intramuscular oxygen-ozone therapy in the treatment of low back pain. Acta Biomed. 2018;89:41–46. doi: 10.23750/ABM.V89I1.5315. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
73. Cantele F., Tognolo L., Caneva F., Formaggio E., Copetti V., Venturin A., Caregnato A., Masiero S. Influence of pain-related psychological factors on therapeutic outcomes in patients with chronic low back pain after oxygen-ozone treatment: A case-series. Eur. J. Transl. Myol. 2021;31:9906. doi: 10.4081/ejtm.2021.9906. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
74. Wong O., Zhang G., Matthews H., Skalski M., Asadi H., Lalloo S., Kurda D. Image-guided spinal injection for pain management. J. Med. Imaging Radiat. Oncol. 2021;66:79–91. doi: 10.1111/1754-9485.13308. [PubMed] [CrossRef] [Google Scholar]
75. Alyan S., Zaghlol R., Mustafa S.A. Efficacy of combined paravertebral ozone (O2O3) therapy with physiotherapy in patients with chronic mechanical low back pain. Egypt. Rheumatol. Rehabil. 2018;45:106–111. doi: 10.4103/err.err_43_17. [CrossRef] [Google Scholar]
76. Sucuoğlu H., Soydaş N. Does paravertebral ozone injection have efficacy as an additional treatment for acute lumbar disc herniation? A randomized, double-blind, placebo-controlled study. J. Back Musculoskelet. Rehabil. 2021;34:725–733. doi: 10.3233/BMR-200194. [PubMed] [CrossRef] [Google Scholar]
77. Cunha C., Teixeira G.Q., Machado C., Pereira C.L., Ferreira J.R., Molinos M., Santos S.G., Barbosa M.A., Goncalves R.M. Modulation of the In Vivo Inflammatory Response by Pro- Versus Anti-Inflammatory Intervertebral Disc Treatments. Int. J. Mol. Sci. 2020;21:1730. doi: 10.3390/ijms21051730. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
78. Andreula C.F., Simonetti L., de Santis F., Agati R., Ricci R., Leonardi M. Minimally Invasive Oxygen-Ozone Therapy for Lumbar Disk Herniation. Am. J. Neuroradiol. 2003;24:996–1000. [PMC free article] [PubMed] [Google Scholar]
79. De Geer C.M. Cytokine Involvement in Biological Inflammation Related to Degenerative Disorders of the Intervertebral Disk: A Narrative Review. J. Chiropr. Med. 2018;17:54–62. doi: 10.1016/j.jcm.2017.09.003. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
80. Li J.-K., Nie L., Zhao Y.-P., Zhang Y.-Q., Wang X., Wang S.-S., Liu Y., Zhao H., Cheng L. IL-17 mediates inflammatory reactions via p38/c-Fos and JNK/c-Jun activation in an AP-1-dependent manner in human nucleus pulposus cells. J. Transl. Med. 2016;14:77. doi: 10.1186/s12967-016-0833-9. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
81. Brisby H. Pathology and possible mechanisms of nervous system response to disc degeneration. J. Bone Jt. Surg. Ser. A. 2006;88:68–71. [PubMed] [Google Scholar]
82. Perolat R., Kastler A., Nicot B., Pellat J.-M., Tahon F., Attye A., Heck O., Boubagra K., Grand S., Krainik A. Facet joint syndrome: From diagnosis to interventional management. Insights Imaging. 2018;9:773–789. doi: 10.1007/s13244-018-0638-x. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
83. Barnabei L., Laplantine E., Mbongo W., Rieux-Laucat F., Weil R. NF-κB: At the Borders of Autoimmunity and Inflammation. Front. Immunol. 2021;2021:3169. doi: 10.3389/fimmu.2021.716469. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
84. Wang B., Wu L., Chen J., Dong L., Chen C., Wen Z., Hu J., Fleming I., Wang D.W. Metabolism pathways of arachidonic acids: Mechanisms and potential therapeutic targets. Signal Transduct. Target. Ther. 2021;6:94. doi: 10.1038/s41392-020-00443-w. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
85. Niu T., Lv C., Yi G., Tang H., Gong C., Niu S. Therapeutic Effect of Medical Ozone on Lumbar Disc Herniation. Med. Sci. Monit. 2018;24:1962–1969. doi: 10.12659/MSM.903243. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
86. O’Neill T.W., McCabe P.S., McBeth J. Update on the epidemiology, risk factors and disease outcomes of osteoarthritis. Best Pract. Res. Clin. Rheumatol. 2018;32:312–326. doi: 10.1016/j.berh.2018.10.007. [PubMed] [CrossRef] [Google Scholar]
87. Vos T., Allen C., Arora M., Barber R.M., Bhutta Z.A., Brown A., Liang X., Kawashima T., Coggeshall M. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386:743–800. doi: 10.1016/S0140-6736(15)60692-4. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
89. Jiang C., Luo P., Li X., Liu P., Li Y., Xu J. Nrf2/ARE is a key pathway for curcumin-mediated protection of TMJ chondrocytes from oxidative stress and inflammation. Cell Stress Chaperon. 2020;25:395–406. doi: 10.1007/s12192-020-01079-z. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
90. de Sire A., Marotta N., Marinaro C., Curci C., Invernizzi M., Ammendolia A. Role of Physical Exercise and Nutraceuticals in Modulating Molecular Pathways of Osteoarthritis. Int. J. Mol. Sci. 2021;22:5722. doi: 10.3390/ijms22115722. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
91. Fernández-Cuadros M.E., Pérez-Moro O.S., Albaladejo-Florin M.J., Alava-Rabasa S. El ozono intraarticular modula la inflamación, mejora el dolor, la rigidez, la función y tiene un efecto anabólico sobre la artrosis de rodilla: Estudio cuasi-experimental prospectivo tipo antes-después, 115 pacientes. Rev. Soc. Esp. Dolor. 2020;27:78–88. doi: 10.20986/resed.2020.3775/2019. [CrossRef] [Google Scholar]
92. Rankothgedera S., Atukorala I., Fernando C., Munidasa D., Wijayaratne L., Udagama P. A potential diagnostic serum immunological marker panel to differentiate between primary and secondary knee osteoarthritis. PLoS ONE. 2021;16:e0257507. doi: 10.1371/journal.pone.0257507. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
93. Chow Y.Y., Chin K.-Y. The Role of Inflammation in the Pathogenesis of Osteoarthritis. Mediat. Inflamm. 2020;2020:8293921. doi: 10.1155/2020/8293921. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
94. Vincent T.L. Mechanoflammation in osteoarthritis pathogenesis. Semin. Arthritis Rheum. 2019;49:S36–S38. doi: 10.1016/j.semarthrit.2019.09.018. [PubMed] [CrossRef] [Google Scholar]
95. Kraus V.B., Karsdal M.A. Osteoarthritis: Current Molecular Biomarkers and the Way Forward. Calcif. Tissue Res. 2021;109:329–338. doi: 10.1007/s00223-020-00701-7. [PubMed] [CrossRef] [Google Scholar]
96. Bar-Or D., Rael L., Thomas G.W., Brody E.N. Inflammatory Pathways in Knee Osteoarthritis: Potential Targets for Treatment. Curr. Rheumatol. Rev. 2015;11:50–58. doi: 10.2174/1573397111666150522094131. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
97. Wang M.-N., Liu L., Zhao L.-P., Yuan F., Fu Y.-B., Xu X.-B., Li B. Research of inflammatory factors and signaling pathways in knee osteoarthritis. Zhongguo Gu Shang. 2020;33:388–392. [PubMed] [Google Scholar]
98. Costa T., Rodrigues-Manica S., Lopes C., Gomes J., Marona J., Falcao S., Branco J. Ozonoterapia na Osteoartrose do Joelho: Revisão Sistemática. Acta Méd. Port. 2018;31:576–580. doi: 10.20344/amp.10330. [PubMed] [CrossRef] [Google Scholar]
99. Sconza C., Leonardi G., Kon E., Respizzi S., Massazza G., Marcacci M., Di Matteo B. Oxygen-ozone therapy for the treatment of low back pain: A systematic review of randomized controlled trials. Eur. Rev. Med. Pharmacol. Sci. 2021;25:6034–6046. doi: 10.26355/eurrev_202110_26881. [PubMed] [CrossRef] [Google Scholar]
100. Barbosa L.T., Rodrigues C.F.D.S., De Andrade R.R., Barbosa F.T. The effectiveness of percutaneous injections of ozonotherapy in low back pain. Rev. Assoc. Méd. Bras. 2020;66:1146–1151. doi: 10.1590/1806-9282.66.8.1146. [PubMed] [CrossRef] [Google Scholar]
101. Hashemi M., Khameneh S.M.H., Dadkhah P., Mohajerani S.A. Effect of Intraarticular injection of ozone on inflammatory cytokines in knee osteoarthritis. J. Cell. Mol. Anesth. 2017;2:37–42. [Google Scholar]
102. Sconza C., Braghetto G., Respizzi S., Morenghi E., Kon E., Di Matteo B. Ultrasound-guided periradicular oxygen-ozone injections as a treatment option for low back pain associated with sciatica. Int. Orthop. 2021;45:1239–1246. doi: 10.1007/s00264-021-04975-w. [PubMed] [CrossRef] [Google Scholar]
103. Iorio G.C., Ammendolia A., Marotta N., Ricardi U., de Sire A. A bond between rheumatic diseases and cancer in the elderly: The interleukin-6 pathway. Int. J. Rheum. Dis. 2021;24:1317–1320. doi: 10.1111/1756-185X.14194. [PubMed] [CrossRef] [Google Scholar]
104. Higashi Y., Sukhanov S., Anwar A., Shai S.-Y., Delafontaine P. Aging, Atherosclerosis, and IGF-1. J. Gerontol. Ser. A. 2012;67:626–639. doi: 10.1093/gerona/gls102. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
105. Tumolo M.R., Panico A., De Donno A., Mincarone P., Leo C.G., Guarino R., Bagordo F., Serio F., Idolo A., Grassi T., et al. The expression of microRNAs and exposure to environmental contaminants related to human health: A review. Int. J. Environ. Health Res. 2020;32:332–354. doi: 10.1080/09603123.2020.1757043. [PubMed] [CrossRef] [Google Scholar]
106. Bromberg P.A. Mechanisms of the acute effects of inhaled ozone in humans. Biochim. Biophys. Acta—Gen. Subj. 2016;1860:2771–2781. doi: 10.1016/j.bbagen.2016.07.015. [PubMed] [CrossRef] [Google Scholar]
107. Arancibia S.E., Zimbron L.F.H., Martinez A.E.R., Maldonado P.D., Perez G.E., Parada M.E. Oxidative stress-dependent changes in immune responses and cell death in the substantia nigra after ozone exposure in rat. Front. Aging Neurosci. 2015;7:65. doi: 10.3389/fnagi.2015.00065. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
108. Huth K., Saugel B., Jakob F., Cappello C., Quirling M., Paschos E., Ern K., Hickel R., Brand K. Effect of Aqueous Ozone on the NF-κB System. J. Dent. Res. 2007;86:451–456. doi: 10.1177/154405910708600512. [PubMed] [CrossRef] [Google Scholar]
109. Renate V.H. Chronic inflammatory processes and the low-dose ozone concept based on the International guidelines of medical ozone: Signal transduction and Bioregulation through «Ozone peroxides» as second Messenger molecules. Медицинский Альманах 2013;3:33. [Google Scholar]
110. Zhang C., Ma S., Zhao X., Wen B., Sun P., Fu Z. Upregulation of antioxidant and autophagy pathways via NRF2 activation protects spinal cord neurons from ozone damage. Mol. Med. Rep. 2021;23:428. doi: 10.3892/mmr.2021.12067. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
111. Delgado-Roche L., Riera-Romo M., Mesta F., Hernández-Matos Y., Barrios J.M., Martínez-Sánchez G., Al-Dalaien S.M. Medical ozone promotes Nrf2 phosphorylation reducing oxidative stress and pro-inflammatory cytokines in multiple sclerosis patients. Eur. J. Pharmacol. 2017;811:148–154. doi: 10.1016/j.ejphar.2017.06.017. [PubMed] [CrossRef] [Google Scholar]
112. Zeng J., Lei L., Zeng Q., Yao Y., Wu Y., Li Q., Gao L., Du H., Xie Y., Huang J., et al. Ozone Therapy Attenuates NF-κB-Mediated Local Inflammatory Response and Activation of Th17 Cells in Treatment for Psoriasis. Int. J. Biol. Sci. 2020;16:1833–1845. doi: 10.7150/ijbs.41940. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
113. Zhang W., Wang F., Zhang L., Sun T., Fu Z. Intrathecal injection of ozone alleviates CCI-induced neuropathic pain via the GluR6-NF-κB/p65 signalling pathway in rats. Mol. Med. Rep. 2021;23:231. doi: 10.3892/mmr.2021.11870. [PubMed] [CrossRef] [Google Scholar]
114. Babaei-Ghazani A., Najarzadeh S., Mansoori K., Forogh B., Madani S.P., Ebadi S., Fadavi H.R., Eftekharsadat B. The effects of ultrasound-guided corticosteroid injection compared to oxygen–ozone (O2–O3) injection in patients with knee osteoarthritis: A randomized controlled trial. Clin. Rheumatol. 2018;37:2517–2527. doi: 10.1007/s10067-018-4147-6. [PubMed] [CrossRef] [Google Scholar]
115. Hedayatabad J.J., Kachooei A.R., Chaharjouy N.T., Vaziri N., Mehrad-Majd H., Emadzadeh M., Abolghasemian M., Ebrahimzadeh M.H. The Effect of Ozone (O3) versus Hyaluronic Acid on Pain and Function in Patients with Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Arch. Bone Jt. Surg. 2020;8:343–354. [PMC free article] [PubMed] [Google Scholar]
116. Hashemi M., Taheri M., Dadkhah P., Hassani H., Ataie M., Ghasemi M., Pourhoseingholi M.A., Solhpour A. Comparison of Two Different Ozone Injection Sites for Knee Osteoarthritis, Tibio-femoral Joint versus Supra-patellar Recess: An Open Randomized Clinical Trial. J. Pharm. Res. Int. 2020;32:37–49. doi: 10.9734/jpri/2020/v32i130393. [CrossRef] [Google Scholar]
117. Raeissadat S.A., Hosseini P.G., Bahrami M.H., Roghani R.S., Fathi M., Ahangar A.G., Darvish M. The comparison effects of intra-articular injection of Platelet Rich Plasma (PRP), Plasma Rich in Growth Factor (PRGF), Hyaluronic Acid (HA), and ozone in knee osteoarthritis: A one year randomized clinical trial. BMC Musculoskelet. Disord. 2021;22:134. doi: 10.1186/s12891-021-04017-x. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
119. Haydt R., Boyle B., Meyers M., Weissberg S., Dyrli K. Comparison of Platelet Rich Plasma and Oxygen Ozone Injections for Knee Osteoarthritis: A Systematic Review. Arch. Phys. Med. Rehabil. 2019;100:e149. doi: 10.1016/j.apmr.2019.08.455. [CrossRef] [Google Scholar]
120. Raeissadat S.A., Tabibian E., Rayegani S.M., Rahimi-Dehgolan S., Babaei-Ghazani A. An investigation into the efficacy of intra-articular ozone (O2–O3) injection in patients with knee osteoarthritis: A systematic review and meta-analysis. J. Pain Res. 2018;11:2537–2550. doi: 10.2147/JPR.S175441. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
121. Cardelli R., de Santis F., Dall’Olio M., Leonardi M. Osteoarthritis of the hip treated by intra-articular infiltration of oxygen-ozone and hyaluronic acid (Hyalubrix®). Preliminary results. Int. J. Ozone Ther. 2008;7:66–69. [Google Scholar]
122. Tartari A.P.S., Moreira F.F., Pereira M.C.D.S., Carraro E., Cidral-Filho F.J., Salgado A.I., Kerppers I.I. Anti-inflammatory Effect of Ozone Therapy in an Experimental Model of Rheumatoid Arthritis. Inflammation. 2020;43:985–993. doi: 10.1007/s10753-020-01184-2. [PubMed] [CrossRef] [Google Scholar]
123. Saraiva L., Konzen V.D.M., Batista J.S., Jorge M.S.G., Garcia G.S., Wibelinger L.M. Treatment of Rheumatoid Arthritis with Ozone Therapy: Systematic Review. Temas Saúde. 2020;20:4–8. doi: 10.29327/213319.20.4-8. [CrossRef] [Google Scholar]
124. Rajaiah R., Puttabyatappa M., Polumuri S.K., Moudgil K.D. Interleukin-27 and Interferon-γ Are Involved in Regulation of Autoimmune Arthritis. J. Biol. Chem. 2011;286:2817–2825. doi: 10.1074/jbc.M110.187013. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
125. Fernández O.S.L., Viebahn-Haensler R., Cabreja G.L., Espinosa I.S., Matos Y.H., Roche L.D., Santos B.T., Oru G.T., Vega J.C.P. Medical ozone increases methotrexate clinical response and improves cellular redox balance in patients with rheumatoid arthritis. Eur. J. Pharmacol. 2016;789:313–318. doi: 10.1016/j.ejphar.2016.07.031. [PubMed] [CrossRef] []
126. Scassellati C., Galoforo A.C., Bonvicini C., Esposito C., Ricevuti G. Ozone: A natural bioactive molecule with antioxidant property as potential new strategy in aging and in neurodegenerative disorders. Ageing Res. Rev. 2020;63:101138. doi: 10.1016/j.arr.2020.101138. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
127. Zeng J., Tang Z., Zhang Y., Tong X., Dou J., Gao L., Ding S., Lu J. Ozonated autohemotherapy elevates PPAR-γ expression in CD4+ T cells and serum HDL-C levels, a potential immunomodulatory mechanism for treatment of psoriasis. Am. J. Transl. Res. 2021;13:349–359. [PMC free article] [PubMed] [Google Scholar]
128. Antonioli L., Blandizzi C., Pacher P., Haskó G. The Purinergic System as a Pharmacological Target for the Treatment of Immune-Mediated Inflammatory Diseases. Pharmacol. Rev. 2019;71:345–382. doi: 10.1124/pr.117.014878. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
129. Ayers N.B., Sun C.-M., Chen S.-Y. Transforming growth factor-β signaling in systemic sclerosis. J. Biomed. Res. 2017;32:3–12. [PMC free article] [PubMed] [Google Scholar]
130. Yagci I., Kenis-Coskun O., Ozsoy T., Ozen G., Direskeneli H. Increased stiffness of median nerve in systemic sclerosis. BMC Musculoskelet. Disord. 2017;18:434. doi: 10.1186/s12891-017-1793-9. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
131. de Sire A., Curci C., Ferrara M., Losco L., Spalek R., Cisari C., Invernizzi M., Solaro C. Efficacy of kinesio taping on hand functioning in patients with mild carpal tunnel syndrome. A double-blind randomized controlled trial. J. Hand Ther. 2021 doi: 10.1016/j.jht.2021.04.011. in press . [PubMed] [CrossRef] [Google Scholar]
132. Elawamy A., Hassanien M., Talaat E.A., Ali A.M., Roushdy A.S.I., Kamel E.Z. Intra-Carpal Injection of Ozone versus Methylprednisolone in Carpal Tunnel Syndrome of Systemic Sclerosis Patients: A Randomized Single-Blind Clinical Trial. Pain Phys. 2021;24:E453–E458. doi: 10.36076/ppj.2021.24.e453. [PubMed] [CrossRef] [Google Scholar]
133. Rascaroli M.W., Borghi B., Rascaroli A., Travagli V. Ozone therapy in idiopathic carpal tunnel syndrome. Biochemical, neurophysiological and clinical aspects. J. Ozone Ther. 2018;2:11286. doi: 10.7203/jo3t.2.3.2018.11286. [CrossRef] [Google Scholar]
134. Rascaroli M., Borghi B. Ozone Therapy in Idiopathic Carpal Tunnel Syndrome. Biochemical, Neurophysiological and Clinical Aspects. J. Ozone Ther. 2019;3:49–50. doi: 10.7203/jo3t.3.4.2019.15530. [CrossRef] [Google Scholar]
135. Bahrami M.H., Raeissadat S.A., Nezamabadi M., Hojjati F., Rahimi-Dehgolan S. Interesting effectiveness of ozone injection for carpal tunnel syndrome treatment: A randomized controlled trial. Orthop. Res. Rev. 2019;11:61–67. doi: 10.2147/ORR.S202780. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
136. Marotta N., Demeco A., Marinaro C., Moggio L., Pino I., Barletta M., Petraroli A., Ammendolia A. Comparative Effectiveness of Orthoses for Thumb Osteoarthritis: A Systematic Review and Network Meta-analysis. Arch. Phys. Med. Rehabil. 2021;102:502–509. doi: 10.1016/j.apmr.2020.06.012. [PubMed] [CrossRef] [Google Scholar]
137. Yamanaka Y., Gingery A., Oki G., Zhao C., Amadio P.C., Yang T.-H. Blocking fibrotic signaling in fibroblasts from patients with carpal tunnel syndrome. J. Cell. Physiol. 2017;233:2067–2074. doi: 10.1002/jcp.25901. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
138. Yang T.-H., Gingery A., Thoreson A.R., Larson D.R., Zhao C., Amadio P.C. Triamcinolone Acetonide affects TGF-β signaling regulation of fibrosis in idiopathic carpal tunnel syndrome. BMC Musculoskelet. Disord. 2018;19:342. doi: 10.1186/s12891-018-2260-y. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
139. Dehlin M., Jacobsson L., Roddy E. Global epidemiology of gout: Prevalence, incidence, treatment patterns and risk factors. Nat. Rev. Rheumatol. 2020;16:380–390. doi: 10.1038/s41584-020-0441-1. [PubMed] [CrossRef] [Google Scholar]
140. Guillén A.G., Karu L.T., Singh J.A., Dalbeth N. Gender and Ethnic Inequities in Gout Burden and Management. Rheum. Dis. Clin. N. Am. 2020;46:693–703. doi: 10.1016/j.rdc.2020.07.008. [PubMed] [CrossRef] [Google Scholar]
141. Bilge A., Tüysüz M., Öztürk Ö., Adali Y., Eroğlu H.A., Makav M., Uslu G.A., Tiskaoglu R. Deneysel Olarak Gut Oluşturulmuş Ratlarda Ozon Terapinin Etkisi. Kafkas Univ. Vet. Fak. Derg. 2019;25:245–249. doi: 10.9775/kvfd.2018.20793. [CrossRef] [Google Scholar]
142. Abdullah D.M., Kabil S.L. Ozone Therapy Alleviates Monosodium Urate Induced Acute Gouty Arthritis in Rats Through Inhibition of NLRP3 Inflammasome. Curr. Drug Ther. 2021;16:345–353. doi: 10.2174/1574885516666210719092523. [CrossRef] [Google Scholar]
143. Saruhanoğlu A., Gökçen-Röhlig B., Saruhanoğlu C., Öngül D., Koray M. Frequency of temporomandibular disorder signs and symptoms among call center employees. CRANIO J. Craniomandib. Pract. 2017;35:244–249. doi: 10.1080/08869634.2016.1216823. [PubMed] [CrossRef] [Google Scholar]
144. Rongo R., Ekberg E., Nilsson I., Al-Khotani A., Alstergren P., Conti P.C.R., Durham J., Goulet J., Hirsch C., Kalaykova S.I., et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for children and adolescents: An international Delphi study—Part 1-Development of Axis I. J. Oral Rehabil. 2021;48:836–845. doi: 10.1111/joor.13175. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
145. Steenks M., Türp J., De Wijer A. Reliability and Validity of the Diagnostic Criteria for Temporomandibular Disorders Axis I in Clinical and Research Settings: A Critical Appraisal. J. Oral Facial Pain Headache. 2018;32:7–18. doi: 10.11607/ofph.1704. [PubMed] [CrossRef] [Google Scholar]
146. Gauer R.L., Semidey M.J. Diagnosis and treatment of temporomandibular disorders. Am. Fam. Phys. 2015;91:378–386. [PubMed] [Google Scholar]
147. Wieckiewicz M., Smardz J., Martynowicz H., Wojakowska A., Mazur G., Winocur E. Distribution of temporomandibular disorders among sleep bruxers and non-bruxers—A polysomnographic study. J. Oral Rehabil. 2020;47:820–826. doi: 10.1111/joor.12955. [PubMed] [CrossRef] [Google Scholar]
148. Manfredini D., Guarda-Nardini L., Winocur E., Piccotti F., Ahlberg J., Lobbezoo F. Research diagnostic criteria for temporomandibular disorders: A systematic review of axis I epidemiologic findings. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011;112:453–462. doi: 10.1016/j.tripleo.2011.04.021. [PubMed] [CrossRef] [Google Scholar]
149. Talaat W.M., Adel O.I., Al Bayatti S. Prevalence of temporomandibular disorders discovered incidentally during routine dental examination using the Research Diagnostic Criteria for Temporomandibular Disorders. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018;125:250–259. doi: 10.1016/j.oooo.2017.11.012. [PubMed] [CrossRef] [Google Scholar]
150. Slade G., Ohrbach R., Greenspan J., Fillingim R., Bair E., Sanders A., Dubner R., Diatchenko L., Meloto C., Smith S., et al. Painful Temporomandibular Disorder: Decade of Discovery from OPPERA Studies. J. Dent. Res. 2016;95:1084–1092. doi: 10.1177/0022034516653743. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
151. Karlsson O., Karlsson T., Pauli N., Andréll P., Finizia C. Jaw exercise therapy for the treatment of trismus in head and neck Cancer: A prospective three-year follow-up study. Support. Care Cancer. 2021;29:3793–3800. doi: 10.1007/s00520-020-05517-7. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
152. Özalp Ö., Yıldırımyan N., Sindel A., Altay M.A., Kişnişci R.Ş. Evaluation of the Short-Term Efficacy of Transdermal Ozone Therapy in Turkish Patients with Internal Derangement of the Temporomandibular Joint. Pesqui. Bras. Odontopediatr. Clín. Integr. 2019;19:1–10. doi: 10.4034/PBOCI.2019.191.44. [CrossRef] [Google Scholar]
153. Fillingim R., Ohrbach R., Greenspan J., Sanders A., Rathnayaka N., Maixner W., Slade G. Associations of Psychologic Factors with Multiple Chronic Overlapping Pain Conditions. J. Oral Facial Pain Headache. 2020;34:s85–s100. doi: 10.11607/ofph.2584. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
154. A Review the Relationship of Bruxism with Temporomandibular Disorders in Children. Syst. Rev. Pharm. 2020;11:136–142. doi: 10.31838/srp.2020.6.22. [CrossRef] [Google Scholar]
155. Seo H., Jung B., Yeo J., Kim K.-W., Cho J.-H., Lee Y.J., Ha I.-H. Healthcare utilisation and costs for temporomandibular disorders: A descriptive, cross-sectional study. BMJ Open. 2020;10:e036768. doi: 10.1136/bmjopen-2020-036768. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
156. Okeson J. Management of Temporomandibular Disorder and Occlusion. 4th ed. Elsevier; Mosby, MO, USA: 1998. pp. 349–380. [Google Scholar]
157. Glaros A.G., Tabacchi K.N., Glass E.G. Effect of parafunctional clenching on TMD pain. J. Orofac. Pain. 1998;12:145–152. [PubMed] [Google Scholar]
158. Fillingim R.B., Ohrbach R., Greenspan J., Knott C., Diatchenko L., Dubner R., Bair E., Baraian C., Mack N., Slade G.D., et al. Psychological Factors Associated With Development of TMD: The OPPERA Prospective Cohort Study. J. Pain. 2013;14:T75–T90. doi: 10.1016/j.jpain.2013.06.009. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
159. Dıraçoǧlu D., Yıldırım N.K., Saral I., Özkan M., Karan A., Özkan S., Aksoy C. Temporomandibular dysfunction and risk factors for anxiety and depression. J. Back Musculoskelet. Rehabil. 2016;29:487–491. doi: 10.3233/BMR-150644. [PubMed] [CrossRef] [Google Scholar]
160. Kellesarian S.V., Al-Kheraif A.A., Vohra F., Ghanem A., Malmstrom H., Romanos G.E., Javed F. Cytokine profile in the synovial fluid of patients with temporomandibular joint disorders: A systematic review. Cytokine. 2016;77:98–106. doi: 10.1016/j.cyto.2015.11.005. [PubMed] [CrossRef] [Google Scholar]
161. de Bont L.G., Stegenga B. Pathology of temporomandibular joint internal derangement and osteoarthrosis. Int. J. Oral Maxillofac. Surg. 1993;22:71–74. doi: 10.1016/S0901-5027(05)80805-7. [PubMed] [CrossRef] [Google Scholar]
162. Sandler N., Buckley M.J., Cillo J., Braun T.W. Correlation of inflammatory cytokines with arthroscopic findings in patients with temporomandibular joint internal derangements. J. Oral Maxillofac. Surg. 1998;56:534–543. doi: 10.1016/S0278-2391(98)90446-3. [PubMed] [CrossRef] [Google Scholar]
163. Tanaka A., Kumagai S., Kawashiri S., Takatsuka S., Nakagawa K., Yamamoto E., Matsumoto N. Expression of matrix metalloproteinase-2 and -9 in synovial fluid of the temporomandibular joint accompanied by anterior disc displacement. J. Oral Pathol. Med. 2001;30:59–64. doi: 10.1034/j.1600-0714.2001.300110.x. [PubMed] [CrossRef] [Google Scholar]
164. Yoshida K., Takatsuka S., Tanaka A., Hatada E., Nakamura H., Nakagawa K., Okada Y. Aggrecanase analysis of synovial fluid of temporomandibular joint disorders. Oral Dis. 2005;11:299–302. doi: 10.1111/j.1601-0825.2005.01120.x. [PubMed] [CrossRef] [Google Scholar]
165. Lv X., Li Q., Wu S., Sun J., Zhang M., Chen Y.-J. Psychological stress alters the ultrastructure and increases IL-1β and TNF-α in mandibular condylar cartilage. Braz. J. Med. Biol. Res. 2012;45:968–976. doi: 10.1590/S0100-879X2012007500102. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
166. Ulmner M., Sugars R., Naimi-Akbar A., Suslu S., Reseland J.E., Kruger-Weiner C., Lund B. Synovial tissue cytokine profile in disc displacement of the temporomandibular joint. J. Oral Rehabil. 2020;47:1202–1211. doi: 10.1111/joor.13051. [PubMed] [CrossRef] [Google Scholar]
167. Son C., Park Y.K., Park J.W. Long-term evaluation of temporomandibular disorders in association with cytokine and autoantibody status in young women. Cytokine. 2021;144:155551. doi: 10.1016/j.cyto.2021.155551. [PubMed] [CrossRef] [Google Scholar]
168. Deregibus A., Ferrillo M., Grazia Piancino M., Chiara Domini M., de Sire A., Castroflorio T. Are occlusal splints effective in reducing myofascial pain in patients with muscle-related temporomandibular disorders? A randomized-controlled trial. Turk. J. Phys. Med. Rehabil. 2021;67:32–40. doi: 10.5606/tftrd.2021.6615. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
169. Vrbanović E., Alajbeg I.Z. Long-term Effectiveness of Occlusal Splint Therapy Compared to Placebo in Patients with Chronic Temporomandibular Disorders. Acta Stomatol. Croat. 2019;53:195–206. doi: 10.15644/asc53/3/1. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
170. Michelotti A., Iodice G., Vollaro S., Steenks M.H., Farella M. Evaluation of the short-term effectiveness of education versus an occlusal splint for the treatment of myofascial pain of the jaw muscles. J. Am. Dent. Assoc. 2012;143:47–53. doi: 10.14219/jada.archive.2012.0018. [PubMed] [CrossRef] [Google Scholar]
171. Armijo-Olivo S., Pitance L., Singh V., Neto F., Thie N., Michelotti A. Effectiveness of Manual Therapy and Therapeutic Exercise for Temporomandibular Disorders: Systematic Review and Meta-Analysis. Phys. Ther. 2016;96:9–25. doi: 10.2522/ptj.20140548. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
172. Ketabi M.A., Sabzijati M. Effect of low-level laser on controlling temporomandibular disorders. Rev. Latinoam. Hipertens. 2020;15:138–143. [Google Scholar]
173. Fertout A., Manière-Ezvan A., Lupi L., Ehrmann E. Management of temporomandibular disorders with transcutaneous electrical nerve stimulation: A systematic review. CRANIO J. Craniomandib. Pract. 2019;9:1–12. doi: 10.1080/08869634.2019.1687986. [PubMed] [CrossRef] [Google Scholar]
174. Yamaner F.E., Celakil T., Roehlig B.G. Comparison of the efficiency of two alternative therapies for the management of temporomandibular disorders. CRANIO J. Craniomandib. Pract. 2020;15:1–10. doi: 10.1080/08869634.2020.1727667. [PubMed] [CrossRef] [Google Scholar]
175. Oshaghi S., Haghighat S. Effectiveness of ozone injection therapy in temporomandibular disorders. Adv. Biomed. Res. 2020;9:73. doi: 10.4103/abr.abr_105_20. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
176. Ávila-Curiel B.X., Gómez-Aguirre J.N., Gijón-Soriano A.L., Acevedo-Mascarúa A.E., Argueta-Figueroa L., Torres-Rosas R. Intervenciones complementarias para el tratamiento de dolor en pacientes con alteraciones temporomandibulares: Una revisión sistemática. Rev. Int. Acupunt. 2020;14:151–159. doi: 10.1016/j.acu.2020.10.004. [CrossRef] [Google Scholar]
177. Ferrillo M., Ammendolia A., Paduano S., Calafiore D., Marotta N., Migliario M., Fortunato L., Giudice A., Michelotti A., de Sire A. Efficacy of rehabilitation on reducing pain in muscle-related temporomandibular disorders: Systematic review and meta-analysis of randomized controlled trials. J. Back Musculoskelet. Rehabil. 2022;1:1–16. doi: 10.3233/BMR-210236. [PubMed] [CrossRef] [Google Scholar]
178. Celakil T., Muric A., Roehlig B.G., Evlioglu G., Keskin H. Effect of high-frequency bio-oxidative ozone therapy for masticatory muscle pain: A double-blind randomised clinical trial. J. Oral Rehabil. 2017;44:442–451. doi: 10.1111/joor.12506. [PubMed] [CrossRef] [Google Scholar]
179. Celakil T., Muric A., Roehlig B.G., Evlioglu G. Management of pain in TMD patients: Bio-oxidative ozone therapy versus occlusal splints. CRANIO J. Craniomandib. Pract. 2019;37:85–93. doi: 10.1080/08869634.2017.1389506. [PubMed] [CrossRef] [Google Scholar]
180. Daif E.T. Role of intra-articular ozone gas injection in the management of internal derangement of the temporomandibular joint. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012;113:e10–e14. doi: 10.1016/j.tripleo.2011.08.006. [PubMed] [CrossRef] [Google Scholar]
181. Doğan M., Doğan D.Ö., Duger C., Kol I.Ö., Akpınar A., Mutaf B., Akar T. Effects of High-Frequency Bio-Oxidative Ozone Therapy in Temporomandibular Disorder-Related Pain. Med. Princ. Pract. 2014;23:507–510. doi: 10.1159/000365355. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
Cranial Neuritis: Therapeutic Effects of Prolotherapy
Cranial neuritis is a condition that is characterized by inflammation or injury to the cranial nerves. Those who are affected by this ailment may experience substantial discomfort and have their normal daily activities disrupted. Prolotherapy is an emerging alternative therapy that should be considered together with the many other treatment alternatives that are now available. In this piece, we will delve into the world of cranial neuritis, investigating its causes as well as its symptoms and the traditional treatments that are available for it. In addition, we will investigate the function that prolotherapy may play in the treatment of cranial neuritis as well as the potential benefits it may offer.
Cranial neuritis is the inflammation or injury of one or more of the cranial nerves. These nerves are responsible for the transmission of sensory and motor information to and from the head and neck. Cranial neuritis can be caused by a number of different conditions. This illness can present itself in a variety of different ways, leading to symptoms such as severe headaches, facial pain, vision changes, dizziness, or hearing difficulties. Cranial neuritis can have a variety of origins, such as bacterial or viral infections, autoimmune diseases, traumatic injuries, or even the result of nerves being compressed.
When a patient has been diagnosed with cranial neuritis, traditional treatment methods are typically implemented. These methods are targeted at lowering inflammation, managing pain, and fostering nerve recovery. Depending on the severity of the condition, they may include anti-inflammatory drugs, pain relievers, physical therapy, or even surgical procedures. Even though these treatments have the potential to alleviate symptoms, they may not always get to the bottom of what's causing the problem or deliver the outcomes that are sought for every person.
Prolotherapy is a minimally invasive method that is gaining prominence as an alternative therapeutic option for a variety of disorders affecting the musculoskeletal system, including cranial neuritis. It is also known by the name regenerative injection therapy. A solution, which is typically a mixture of dextrose or another irritating material, is injected directly into the area that is afflicted as part of the procedure. The purpose of the solution is to activate the body's natural healing reaction, so facilitating the restoration of injured tissues, ligaments, and tendons and enhancing their strength.
Individuals who are diagnosed with cranial neuritis may stand to profit from prolotherapy in a number of different ways, according to proponents of the treatment. First, the goal of prolotherapy is to regenerate damaged nerves by activating the natural healing mechanisms of the body. This, in turn, should promote nerve repair and reduce inflammation. It is possible that patients will experience less pain as a result of this, as well as improved function and an overall improvement in their quality of life.
Additionally, due to the regenerative properties of prolotherapy, it may be possible to address the underlying causes of cranial neuritis, thereby addressing the issue at its source rather than merely treating the symptoms. Prolotherapy may be able to assist treat the structural imbalances or weaknesses that are contributing to nerve inflammation and irritation. It does this by encouraging the healing and strengthening of tissue.
Cranial neuritis can have a substantial negative impact on a person's health by creating symptoms that are incapacitating and by interfering with daily life. Exploring alternative treatments such as prolotherapy, which may give new alternatives for the management of cranial neuritis, while conventional treatments provide relief for many people who suffer from cranial neuritis. Prolotherapy has the ability to enhance nerve healing, reduce inflammation, and correct underlying structural imbalances due to its regenerative nature. However, it is absolutely necessary to confer with medical experts in order to ascertain whether or not prolotherapy is appropriate for a particular patient's condition and whether or not it is likely to be beneficial.
The office of Dr. Alvin Philipose can be reached at (405) 848-7246.
Autoimmune diseases are difficult conditions characterized by a hyperactive immune response against the body's own tissues. Mast cells, vital immune system components, have been found to play a significant role in the onset and progression of autoimmune diseases. Ozone therapy has emerged as a possible therapeutic option as researchers continue to investigate alternative therapies. In this article, we will examine the relationship between mast cells and autoimmune diseases, as well as the use of ozone therapy as a novel method for their treatment.
Understanding Mast Cells and Immune System Disorders
Mast cells are immune cells that are predominantly found in tissues that come into contact with the external environment, such as the epidermis, respiratory system, and digestive system. They possess receptors capable of recognizing pathogens, allergens, and other triggers. In autoimmunity, mast cells can become hyperactive and cause the excessive release of histamine, cytokines, and other inflammatory mediators, resulting in chronic inflammation and tissue injury.
Mast cells have been implicated in a variety of autoimmune diseases, including:
Mast cells are present in the synovial fluid and tissue of affected joints in patients with rheumatoid arthritis. Their activation contributes to the inflammatory response and joint degeneration characteristic of this condition.
Mast cells participate in the immune response in Systemic Lupus Erythematosus (SLE) and are associated with the release of autoantibodies and pro-inflammatory molecules, thereby exacerbating tissue injury and organ involvement.
Mast cells serve a role in the neuroinflammatory processes of multiple sclerosis (MS). Their activation may contribute to the collapse of the blood-brain barrier and the infiltration of immune cells into the central nervous system.
Ozone Therapy: A Different Method
Alternative medicine ozone therapy entails the administration of ozone gas to promote healing and modulate the immune system. Ozone is a highly reactive form of oxygen that may have anti-inflammatory, immunomodulatory, and antimicrobial effects on the body. Here are the potential benefits of ozone therapy in the context of autoimmune diseases and mast cell involvement:
It has been discovered that ozone therapy modulates mast cell activation and reduces the release of inflammatory mediators such as histamine and cytokines. Ozone therapy may alleviate the chronic inflammation associated with autoimmune diseases by modulating mast cell function.
It has been demonstrated that ozone therapy decreases the production of pro-inflammatory molecules while increasing the production of anti-inflammatory substances. This change in the immune response has the potential to assist in regulating the excessive inflammation observed in autoimmune diseases.
Immune System Regulation Ozone therapy has immunomodulatory effects, which means it can balance and regulate immune system activity. By fostering a balanced immune response, ozone therapy may prevent the immune system from attacking healthy tissues, which is a defining characteristic of autoimmune diseases.
Enhanced Oxygen Utilization Ozone therapy can enhance the cellular oxygen utilization. Improved oxygen delivery and utilization can support tissue repair and boost overall cellular function, which may be advantageous for autoimmune patients.
While ozone therapy shows promise as an alternative treatment, more research is required to ascertain its safety, efficacy, and optimal protocols for treating various autoimmune conditions. To ensure appropriate administration and monitoring, it is vital to consult with a qualified healthcare professional at Venturis in Oklahoma City with experience in ozone therapy.
Ozone therapy has been gaining popularity in recent years as a natural and non-invasive treatment option for a variety of health conditions. It involves the administration of ozone gas, which is made up of three oxygen atoms, to the body to improve oxygen delivery and promote healing. However, many people are not aware that there are different types of ozone therapy available. In this blog post, we'll explore the different types of ozone therapy and what they are used for.
Major Autohemotherapy (MAH)
Major Autohemotherapy (MAH) is one of the most common types of ozone therapy. It involves withdrawing a small amount of the patient's blood, mixing it with ozone, and then reintroducing the ozonated blood back into the patient's bloodstream. This type of therapy is used to improve circulation, boost the immune system, and promote healing.
Rectal Insufflation
Rectal insufflation is a type of ozone therapy that involves the administration of ozone gas through the rectum. This method is typically used to treat digestive disorders, such as irritable bowel syndrome, and to improve overall gut health.
Ozone Sauna Therapy
Ozone sauna therapy involves the use of a special sauna that infuses ozone gas into the air. The patient sits in the sauna and inhales the ozonated air, which is believed to improve circulation, boost the immune system, and promote detoxification.
Ozonated Water
Ozonated water is created by bubbling ozone gas through water, which creates ozonated water. This type of therapy is typically used to treat skin conditions, such as eczema and acne, and to promote overall skin health.
Ozone Injection Therapy
Ozone injection therapy involves the direct injection of ozonated saline into specific areas of the body, such as joints or muscles. This type of therapy is typically used to treat pain and inflammation.
Bagging
Bagging is a type of ozone therapy that involves placing a plastic bag over a specific area of the body, such as a limb, and infusing ozone gas into the bag. This method is typically used to treat wounds, infections, and skin conditions.
It's important to note that while ozone therapy is generally safe, there are some risks associated with the treatment. Patients should speak with a healthcare provider to determine if ozone therapy is right for them and which type of therapy would be best for their specific health concerns.
Ozone therapy is a natural and non-invasive treatment option for a variety of health conditions. There are different types of ozone therapy available, each with its own specific uses and benefits. Patients should speak with a healthcare provider at Venturis Clinic in Oklahoma City to determine which type of ozone therapy would be best for their individual needs.
If you have tried multiple types of doctors and treatments but still hurting, you may not have found the cause. We can help!
The Venturis Chiropractic and Prolotherapy website uses cookies, tracking pixels and related technologies. By continuing to browse our site, you are agreeing to our use of cookies. OkPrivacy policy

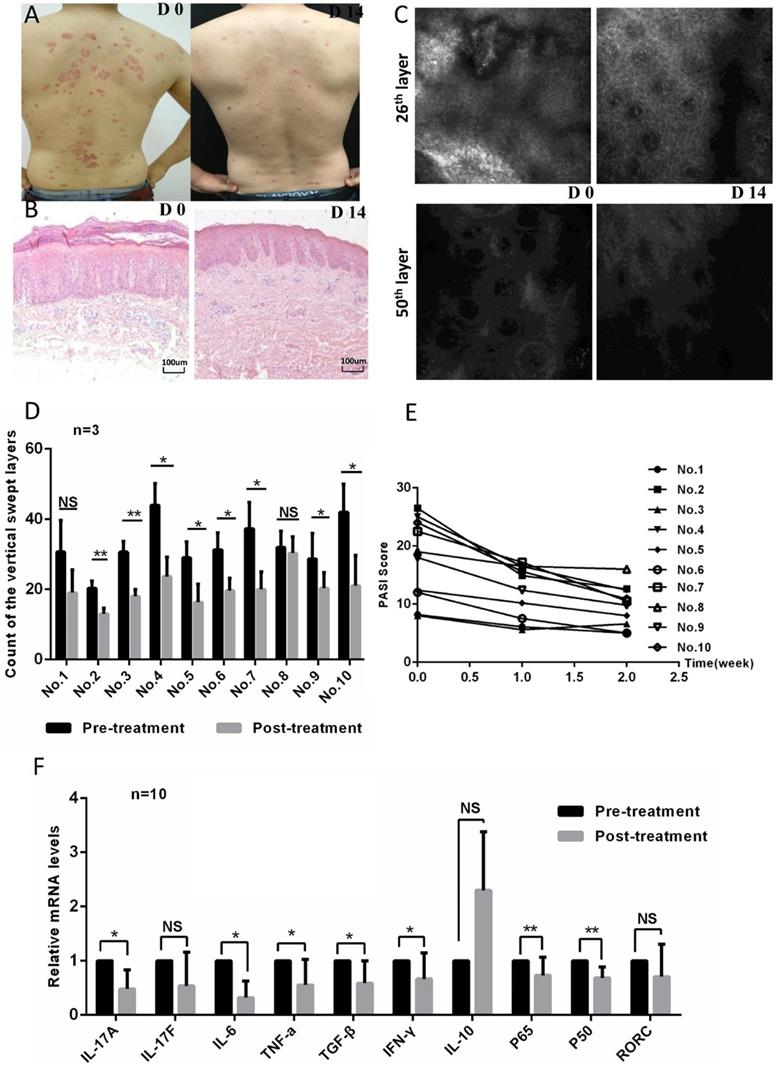
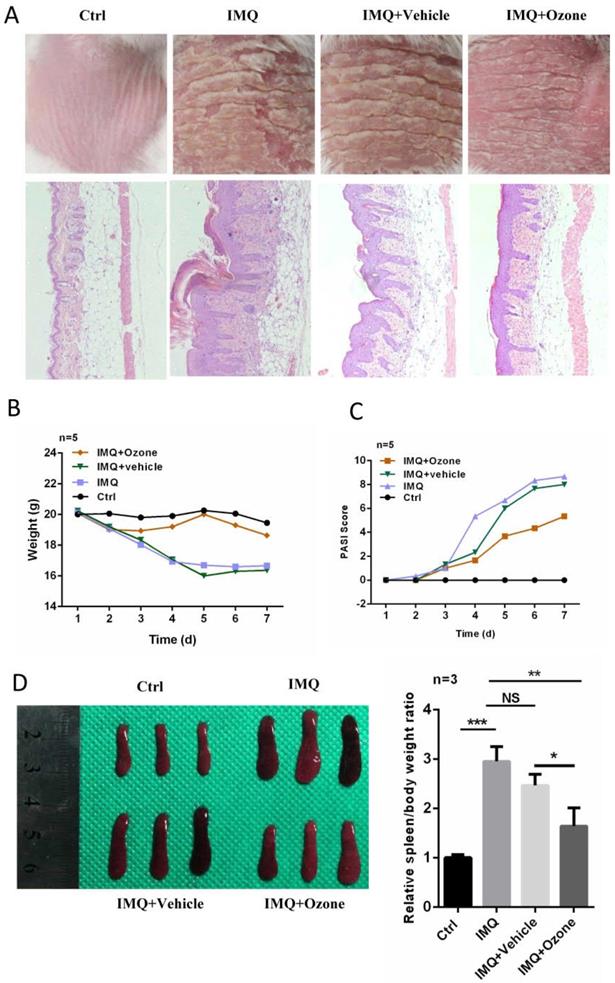
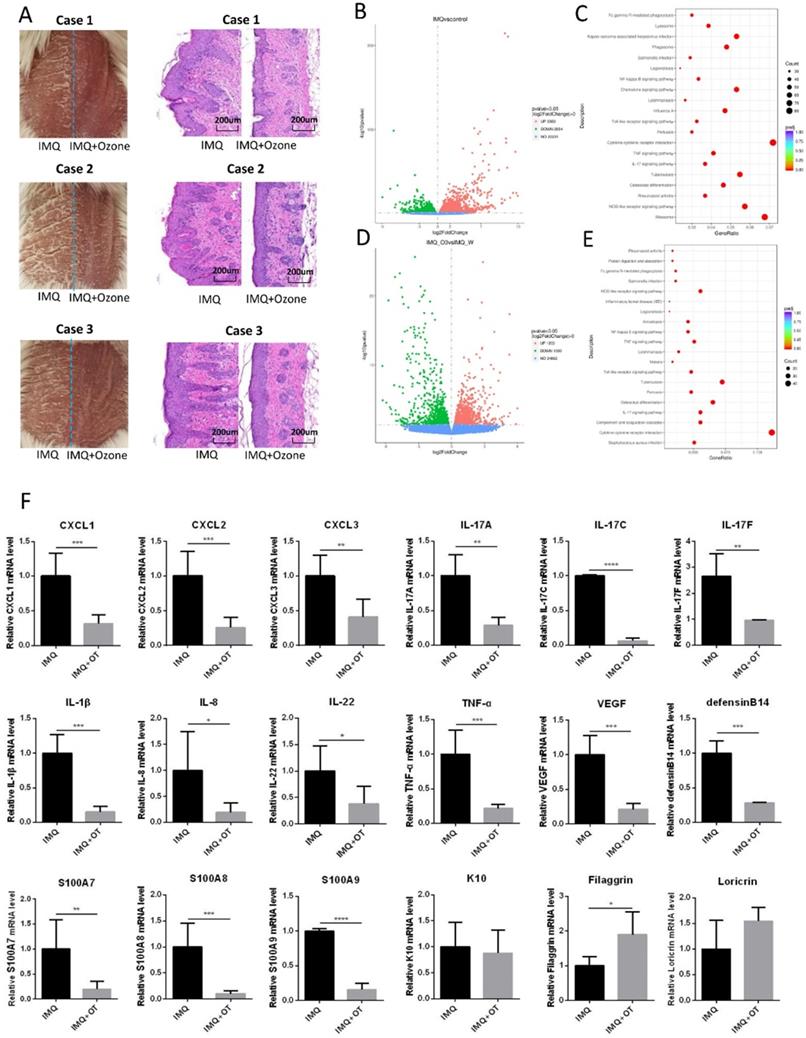
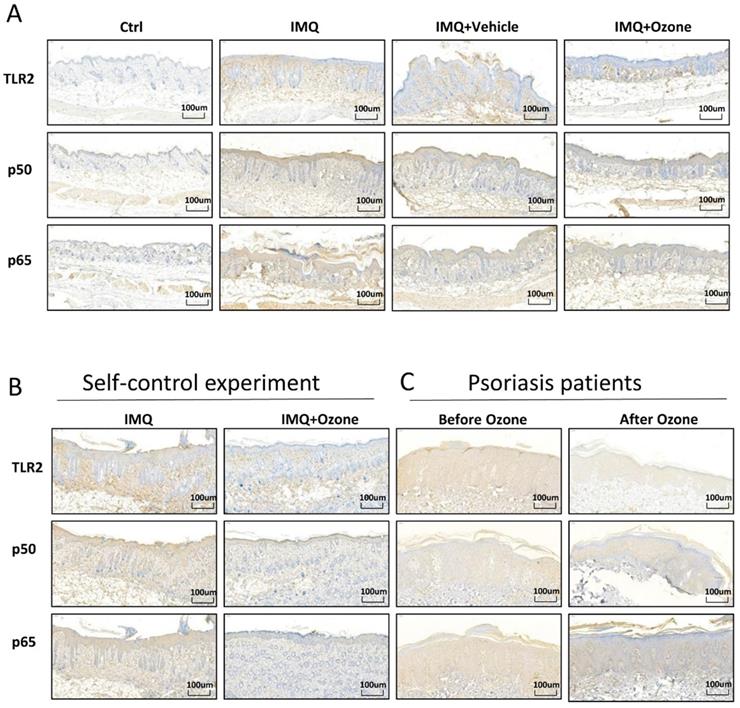
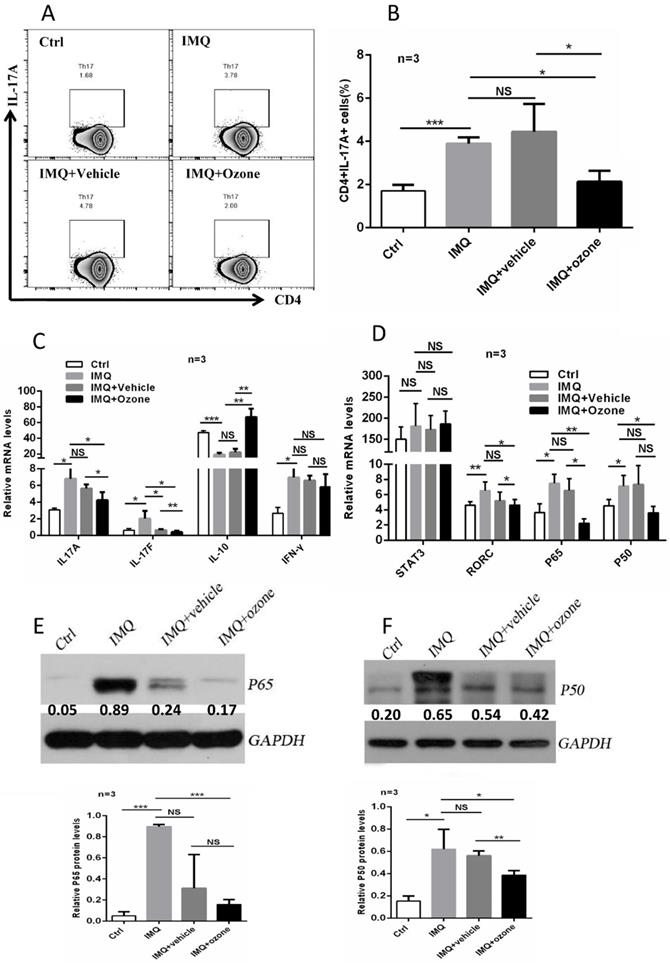
 Francisco Javier Hidalgo-Tallón
Francisco Javier Hidalgo-Tallón Luis Miguel Torres-Morera2
Luis Miguel Torres-Morera2 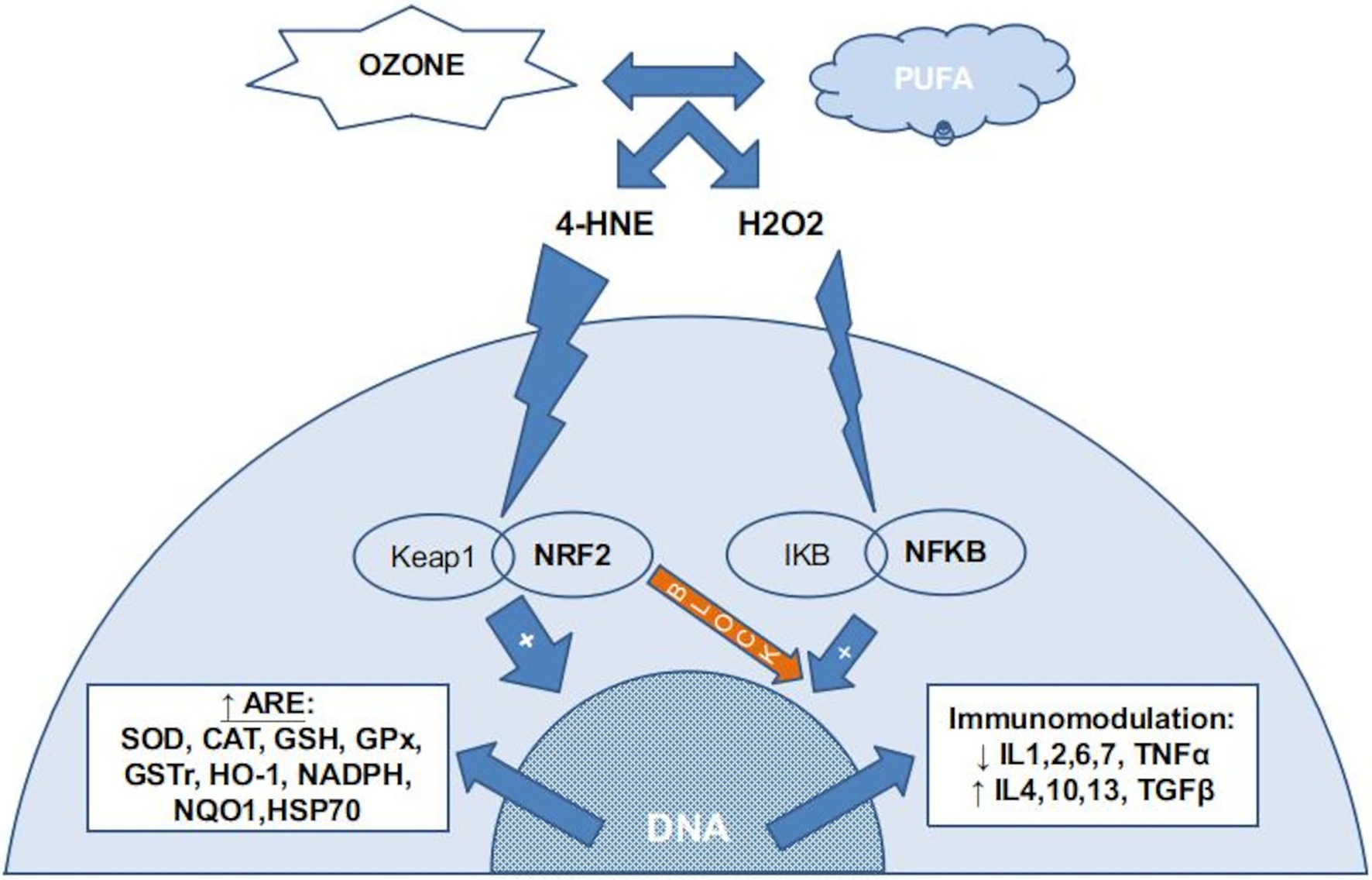 FIGURE 1. The chemical reaction between ozone and PUFA (poli-unsaturated fatty acids) in the insterstitial water (or plasma) produce several ROS, mainly H2O2, and several LOPs, mainly 4-HNE (4-hydroxynonenal). Almost all H2O2 is kidnaped by erythrocytes (not reflected in this figure) if present. In nucleated cells, LOPs activates the NRF2 pathway, inducing the production of ARE (antioxidant response elements) and blocking the NFKB pathway. A small amount of H2O2 stimulates the NFKB pahtway, usually balanced with the NRF2 blocking action, producing a inmmunomodulation.
FIGURE 1. The chemical reaction between ozone and PUFA (poli-unsaturated fatty acids) in the insterstitial water (or plasma) produce several ROS, mainly H2O2, and several LOPs, mainly 4-HNE (4-hydroxynonenal). Almost all H2O2 is kidnaped by erythrocytes (not reflected in this figure) if present. In nucleated cells, LOPs activates the NRF2 pathway, inducing the production of ARE (antioxidant response elements) and blocking the NFKB pathway. A small amount of H2O2 stimulates the NFKB pahtway, usually balanced with the NRF2 blocking action, producing a inmmunomodulation.
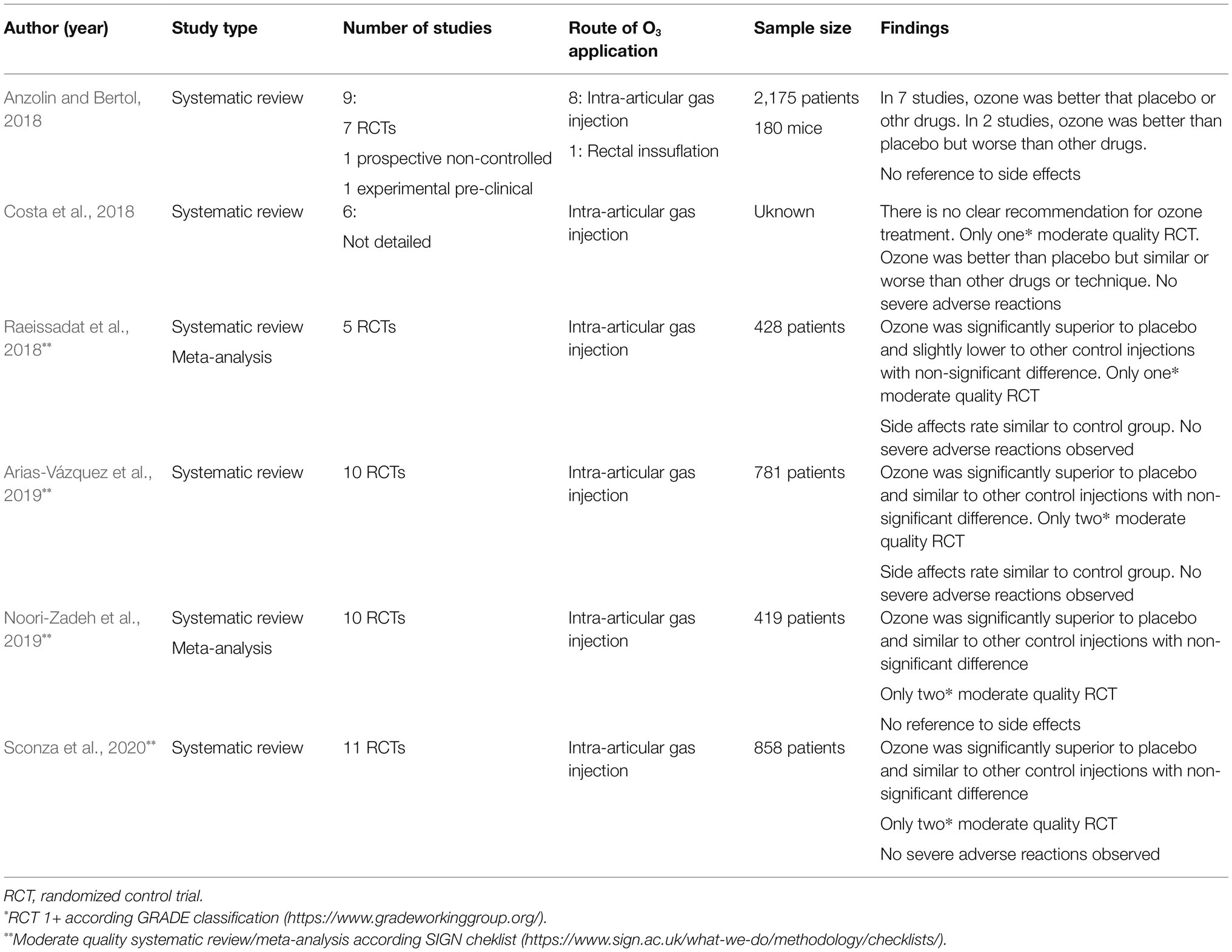 TABLE 1. Systematic reviews and meta-analysis on medical ozone in knee osteoarthritis (Anzolin and Bertol, 2018; Costa et al., 2018; Raeissadat et al., 2018; Arias-Vázquez et al., 2019; Noori-Zadeh et al., 2019; Sconza et al., 2020).
TABLE 1. Systematic reviews and meta-analysis on medical ozone in knee osteoarthritis (Anzolin and Bertol, 2018; Costa et al., 2018; Raeissadat et al., 2018; Arias-Vázquez et al., 2019; Noori-Zadeh et al., 2019; Sconza et al., 2020).


